Attachmentis the “emotional bond” between a child and their caregiver. It’s relevant to personality disorders since it influences the child’s “capacity to form mature intimate relationships in adulthood”. It “influences and organizes motivational, emotional, and memory processes that involve caregivers”. Attachment is associated with “emotional regulation, social relatedness” and the “developmentofself-reflection and narrative”, all things that are impacted by personality disorders.
Attachment Styles
Attachment styles are made up of two dimensions:
thedistinction between self and others
“valence”:positive vs. negative evaluation
Most people will exhibit more than one attachment style.
Thefive stylesare:
secure:positiveview of self and others
preoccupied:negativeview of self,positiveview of others
dismissing:positiveview of self,negativeview of others
fearful:negativeview of self and others
disorganized:fluctuatingpositive and negative views of self and others
Preoccupied style: DPD, OCPD & HPD
Negativeview of self(“a sense of personal unworthiness”)
Positiveview of others
Tend to be very “externally oriented in their self-definitions”, i.e. look to others to define them
Dismissing style: SZPD
Positiveview of self(“a sense of self that is worthyandpositive”)
Negativeview of others, which “typically manifests as mistrust”
See themselves as “emotionally self-sufficient”
See others as emotionally unresponsive
Therefore they “dismiss the need for friendship and contact with others”
Fearful style: PPD
Negativeview of selfandothers
Expectationthat others are untrustworthy & will rejectthem
As promised, Anon, here’s a VERY quick and dirty rundown of disorganized attachment and the role it plays in the development of dissociation. Sorry it took so long ;–; This doesn’t even begin to cover it, but I hope it at least gives people a basic understanding.
Please remember, this is so incredibly brief and barely scratches the surface. It’s a really interesting field of research, and it has a lot of important (and good!) implications to therapy techniques and models. I highly encourage people that are interested to look through some of the below resources, or make a request for any specific aspects you want discussed further. Apparently, left to my own devices with a broad topic, I fail to be coherent.
What is disorganized attachment (DA)?
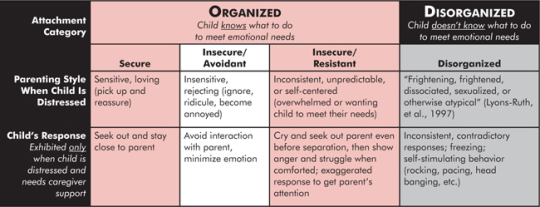
There are technically 4 types of attachment between a child and caregiver, differentiated by response patterns. The first 3 types (secure, insecure-avoidant, and insecure-ambivalent) are considered forms of “organized attachment”, despite the negative behaviours associated with it, because even if they’re not “secure”, the behaviour patterns are still organized and, more importantly, consistent. In other words, in all 3 types of organized attachment, the child knows exactly what they need to do to meet their emotional needs, and the patterns in their behaviour are considered organized.
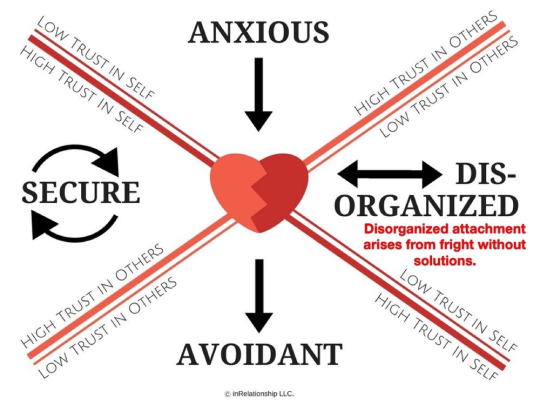
In DA, though, the child is confused, and there’s no pattern to their behaviour. They’re torn between wanting to flee to, and flee from the caregiver. When a caregiver is unpredictable and traumatizing, the child has a difficult time establishing a consistent view of the caregiver, and of themselves. In other words, the caregiver is both needed, and someone to be avoided, and the child may not understand what makes them a “good” or “bad” child, as the caregiver’s behavior is often confusing and unpredictable.
It’s summed up quite well in this image:
What causes disorganized attachment?
All the same standard things you would already know about. Abuse, neglect, behaviour that’s frightening, intrusive or insensitive, and disrupted affective communication, but it really boils down to, “A parent’s consistent failure to respond appropriately to their child’s distress, or by a parent’s inconsistent response to their child’s feelings of fear or distress.” And this happens in childhood. The way a baby or very young child form attachments are the base building blocks that a child will use to build their relationships with people in the future.
It’s important to note that it’s not just abuse that can cause a child to form DA. Sometimes loving caregivers who have experienced trauma themselves can behave in confusing ways toward the child, especially if they are suffering untreated PTSD or DID themselves. This happens because of the caregiver’s own inability to control their emotions. Traumatized parents can have a difficult time managing their emotions and providing a sense of security for the child even though they are not abusive or neglectful. Anger or fear can erupt unexpectedly and traumatize the child.
As well, “Disorganized attachment is often the result of intergenerational parenting patterns. This means parents are responding to their children in the same unhealthy ways their own parents responded to them when they were children.”
What role does disorganized attachment play in dissociation?
This one is… A bit tough. There’s a lot of factors in play and so much ground to cover.
First, when discussing dissociation, it’s talking about it in a general sense. Everyone is capable of dissociating, and it’s simply when you become detached from reality in response to trauma– at any age, for any kind of traumatic event. It’s also important to note that without a secure attachment style, an overwhelmingevent is more likely to be perceived as trauma. Basically, though, dissociation is a general symptom in this regard, not specific to any single disorder. DA is linked to dissociation, and from there, combined with othersymptoms someone may be experiencing, it can become problematic and be assigned to specific mental disorders.
So, the child needsto maintain a relationship with the caregiver– they have no one else to turn to, so the child can develop dissociation as a way to make sense of themselves, and to maintain a child-caregiver relationship. They may “forget” the abuse, or deny it. “It is an adaptive and defensive strategy that enables the child to function within the relationship, but it often leads to the development of a fragmented sense of self.” This fragmented sense of self may or may not develop into something worse– namely, BPD and DID based on severity, frequency, and whether there was any sense of reprieve (i.e. a child can avoid the worst of dissociative symptoms if one of their parents was more supportive, because it helps them build some positive attachments).
Children with DA and suffering from abuse “are likely to generate two or more dissociated self states, with contradictory working models of attachment,” in order to handle their confusing relationship with the caregiver. From there, “It is proposed that the propensity to react to traumatic events with dissociation is related to disorganization of early attachment and its developmental sequelae.” This is fundamentally the basis of why DID can’t form once the child creates an integrated sense of self. It is theorized that DA and dissociative disorders are inexplicably linked together. You can have DA and not develop DID/OSDD, but you can’t have DID/OSDD without DA.
A lot of new research is suggesting that it’s not so much trauma as we know it (physical and sexual abuse) that is linked to dissociation, but that traumais something that is far more discrete and insidious (longterm inconsistent and confusing parenting styles linked to DA) and that it’s only part of “a complex web of environmental, societal, familial, and genetic factors that are all likely to interact in ways that we have only begun to understand.” This is something I firmly believe in and attribute to a lot of the endogenic claims of having no trauma (and under this theory, “overwhelming events” also constitute trauma).
Interestingly, it’s theorized that different types of attachment are linked to different mental disorders. “Attachment insecurity can therefore be viewed as a general vulnerability to mental disorders, with the particular symptomatology depending on genetic, developmental, and environmental factors.” Going back to the 4 types of attachment, the 3 insecure types can be linked to basically all types of disorders. They are all linked to depression, anxiety, OCD, PTSD, eating disorders and suicidal tendencies, but those with anxious attachment are more likely to develop things like DPD, HPD and BPD and are drawn to co-dependent relationships. Those with avoidant attachment are more likely to develop things like SPD and APD and form addictive habits, and those with disorganizedattachment are more likely to develop DID/OSDD.