/* The Superiority Complex Defence Mechanism Disorder of each cluster <3 [ Just a tongue-in-cheek meme, not a statement of every single person with these disorders ]
… That said, here’s a breakdown of the feelings of superiority of these three disorders and how they differ. As usual, these are general frameworks. Actual individuals may not have all these traits/have different ones, or may have overlapping ones [ especially, but not necessarily, if they are comorbid ].
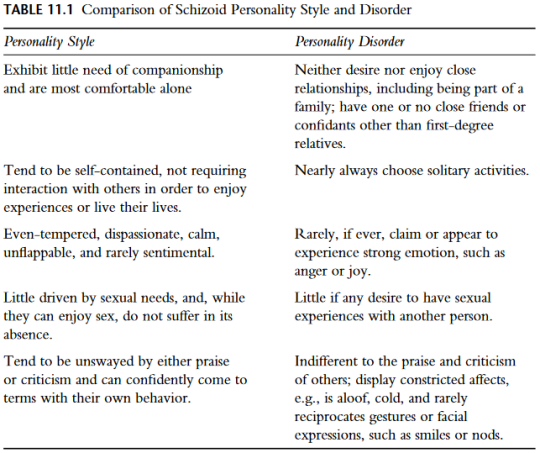
Schizoid Personality Disorder
Goal:Safety
Defence against: Feelings of intrusion
Manifests as: Doing everything alone, secrecy [ to avoid other people’s input and thus “control” of their decisions ], unclear goals and expectations of both themselves and others, distaste for emotions and seeing it as “dramatic”, distaste for people and refusal to be in relationships
Differences from NPD and OCPD: Does not tend to impose their own standards/expectations on others [ preference to avoid people altogether ]; does not seek outward validation/may be uncomfortable with positive acknowledgement and reassurance, relatively more apathetic to failureand criticism [ may feel unaffected or unconsciously shut down negative emotions ]; tendency to give up more easily
People with ScPD, due to their detachment from emotions and preoccupation with thoughts, are often more adept at objectively assessing the thoughts and behaviour of other people. Coupled with their buried hypersensitivity to emotions, this often leads the schizoid to see others as dramatic and sometimes stupid.
In reality, the schizoid may not necessarily genuinely see themselves as a “great” person [ although seeing themselves as “incompetent” is not necessary either ]: rather, their apprehension towards other people [ or specifically, emotions, both other people’s and their own ] leads them to adopt a “superiority complex” as a method of protecting the self. The schizoid learns to be hyper-independent, convincing themselves they are capable of doing everything alone to avoid the need to ask for help, disclosing their emotions to others or entering relationships as much as possible.
The schizoid’s mechanism of shutting down their own emotions due to the inability to handle them leads to a mindset where emotions are seen as a “frivolous” thing, and other people who more readily display them may be devalued for this reason.
Unlike people with NPD, who are more likely to want to show their competency to other people, the schizoid prefers to keep things to themselves, and may be unwilling to share things they are genuinely passionate about/good at [ for example, works of art ] due to the belief the perception/input of others are intrusive and controlling.
People with ScPD often feel “helpless” and unable to control their situation similar to those with OCPD. However, they respond by shutting down their emotions in general and passively accepting things as they are. They may often think that reacting to things “dramatically” is beneath them.
Maladaptively, this leads to struggles in relationships because the schizoid often has difficulty sympathising with other people, and may find their genuine attempts at kindness annoying or even dangerous. The schizoid may also be unable to manage their own tasks or needs alone due to the inability to disclose their emotions, ask for help or commit to things that are too difficult.
Narcissistic Personality Disorder
Goal:Self-worth
Defence against: Feelings of worthlessness
Manifests as: Desire to “prove” self to others, taking on leadership roles, comparison with or devaluation of other people, extreme reaction to failure and criticism, high need for admiration
Differences from ScPD and OCPD: More willing to form relationships or work with others [ especially to achieve validation ]; often has genuine (if nebulous/volatile) confidence in their own capabilities; better decisiveness and ability to finish the tasks they set out to do [ People with ScPD may be too apathetic/anhedonic/unmotivated to have clear goals, people with OCPD may be too preoccupied with doing things a certain way to be efficient ]; tendency to feel negative judgments about them are undeserved/incorrect; higher tendency to change their preferences, standards, behaviour, etc. in accordance to what others expect
People with NPD often feel the need to be admirable due to an ingrained belief that this is the only way they can be worthy of love.
As such, they will often take on tasks with the aim of “proving” they are “worthy” of admiration. Unlike the schizoid who prefers to keep things to themself, the narcissist will often want to display the things they are good at in order to receive validation from others.
This can lead to them wanting prominent roles in their endeavours, or actively seeking out relationships with others to receive validation or to have somebody to “prove” their competency to.
Similar to those with OCPD, they are sensitive to criticism. However, unlike people with OCPD who may obsessively feel the need to “fix” themselves and adhere closer to rigid rules to escape reproach, people with NPD may instead devalue other people’s opinions or to shift their goals/standards to deflect the feeling of “falling short.”
Maladaptively, they may devalue or put down other people, which can lead to struggles in maintaining relationships or cause conflicts among others. They may also take on more work than they are capable of due to overestimation of their own abilities and/or the desire to prove their own competency to others, leading to burnout and exhaustion. They may be ill-equipped to handle the feelings of insecurity and shame that come with failure or criticism, which can be the cause of other more maladaptive behaviour such as intense withdrawal, lashing out or self-destructive habits.
Obsessive-Compulsive Personality Disorder
Goal:Control
Defence against: Feelings of helplessness
Manifests as: Doing everything alone, preoccupation with what they do/how to do so, imposing rigid rules on others, extreme reaction to failure and criticism, high need for validation
Differences from ScPD and NPD: Higher or more rigid standards/rules/processes of how things “should” be navigated; tendency to get “stuck” on the same goal or to keep abiding to the same standards to their detriment [ People with ScPD will tend to abandon things instead, people with NPD may feel confident enough in their own work to have a decisive “finish line” or will change their goals/standards to better suit what they are already doing ]
People with OCPD feel a higher level of anxiety than most people, and thus adopt the “superiority complex” to combat this. Like people with NPD, people with OCPD tend to be more sensitive to failure and criticism, and their adherence to strict standards is often due to the belief that other people will have nothing to criticise them for if they are able to perform “perfectly” enough.
People with OCPD often have rigid standards of behaviour, whether it comes to their ethical standards, the process of which tasks must follow, or the rules people must abide to. They often want to do their tasks in only a specific way, and like the schizoid will often want to do everything by themself due to believing other people will only slow them down. However, while people with ScPD may primarily believe others are too emotional/frivolous, but not necessarilyincompetent, people with OCPD may be more critical of how others perform due to wanting them to abide to their personal standards.
Similar to people with ScPD, people with OCPD often feel a high sense of obligation and responsibility to the things around them and are made to feel helpless because of this. Unlike the schizoid who responds to this by avoidance and passivity, people with OCPD are more likely to “redirect” the feeling into certain tasks [ or the way these tasks are performed ], in order to regain a sense of having control/influence over their situation.
The belief that there is an undeniably “correct” way to do things makes OCPD somewhat similar to OCD [ of which the comorbidity rates are higher than that with other personality disorders ], however they are not the same due to the lack of egodystonic obsessions/compulsions that present the way they do in OCD.
Maladaptively, their rigid standards can make relating to others difficult as they may become critical or distrustful of others for not understanding or complying with their expectations. They may also often struggle with inefficiency, due to the inability to follow their own standards or the preoccupation with perfectionism. The belief that their own method of living is superior makes unfamiliar situations highly distressing.
Traits in Common
Low/no empathy; downplaying of other people’s emotions
Difficulty assessing the effect they have on other people; either overestimating or underestimating the depth of their relationships, or vacillating between doing the two
Difficulty trusting other people, which often leads to hyper-independence[ NPD: Higher tendency to work with others but may want to take on leadership roles/decide who does what ]
Difficulty disclosing their genuine emotions due to fear of being perceived negatively [ ScPD: Fear of people interfering in an attempt to “help”; NPD: Fear of being seen as incompetent and unworthy of love/relationships; OCPD: Fear of losing their “grasp” of themselves/their circumstances and being subjected to the criticism or demands of others ]
Desire for an extreme degree of control over their own circumstances; difficulty accepting the input of others [ ScPD: Less negative reaction to criticism, but still unlikely to actually put it into practice due to apathy or devaluation of other people’s opinions ]
Repetitive and stagnated tasks/habits; inability to try new things [ ScPD: Apathy/anhedonia/avolition and refusal to ask for instruction makes the schizoid unlikely to have clear goals; NPD/OCPD: Fear of failure and criticism makes them unlikely to do something if they are not certain they can do it well ]
I started therapy on the 23d of July 2019. I was 35 years old at the time, and I had decided to go into therapy for the following reasons:
I felt permanently exhausted
I felt like somewhere during my adult years I had slipped into a depression I’d never gotten out of and I wanted to feel happier in life than I did at that time
executive dysfunction - I still need regular help from my mom to keep my household in order
I lacked any and all ambition to do anything with my life
I had begun to suffer from anxiety and sometimes tiny anger outbursts which were occuring more often than before, which was a sign to me something was wrong and only getting worse as I aged.
I had tried seeing a psychologist when I was 30. It was a man who I disliked so much that after 2 sessions, I ghosted him. I could go into more details, but let’s just say he was not a match for me.
It took me five years before I gathered enough energy and courage to try again. In a way, Tony Atwood helped. I’d stumbled across his videos on Aspergers in women and I’d begun to think that maybe it was Aspergers then. The above symptoms would not be misplaced in a women my age with Asperger - and it was until I got my diagnosis two weeks ago, on the 8th of May, that I was bracing myself for an Asperger diagnosis.
When it turned out to be Schizoid Personality Disorder, I was like: “I’m a what now?”
But kudos to Tony Atwood’s videos for at least encouraging me to seek help and to approach a possible diagnosis with optimism. Even if it’s not Aspergers, I needed that little push in the back.
After nearly a month, I’ve returned with another blog post.
I’ve had a few interesting therapy sessions in the meanwhile. It turns out I’ve also got severe depression along with my schizoid personality disorder. Next session we’re starting with EMDR – which is eh… something I don’t fully understand myself - yet. I’ll gladly talk more about it once I have a better idea of what it actually does. It sounds a little bit like hypnosis, but not fully, and it would probably be considered an insult to the practitioner to label it as hypnosis. I might write about it in an upcoming blog post.
But for today, I’d prefer to stick to a topic I understand better. Solitude. Loneliness. The two are not the same for many schizoids.
The shortest way in which I can put it, is to say that many schizoids don’t experience loneliness when they’re alone. But they might feel it when they’re in a group.
If you’re a schizoid who feels like “the walking dead”, this might mean you dissociate. A lot. And apparently, for schizoids, that’s common.
Others might not know what dissociating is, or might think “oh I dissociated” the moment they miss one point during a meeting. (Yes, that’s dissociation, but not to the extent a schizoid experiences it.)
Dissociation is a way to protect us from harm and strong emotions, but it also makes our lives bleaker. Dissociation is like living in a house where the temperature is always steady, but because of this, you do not know what hot or cold is. Or even worse: when it suddenly does get hot or cold, it’s suddenly a disaster because you never experienced it, and you go through some panic because of it and dissociate again as soon as you are possible.
Today’s blog post is about this common aspect of SPD and the goal is to explain what it is, where it comes from, how Schizoids vs. Neurotypicals might experience this, what can be done to dissociate less. Finally, it poses the question whether this is a blessing or a curse. I’ll also be giving a personal example of a recent time I was about to dissociate and was able to catch myself in the moment (thanks to therapy.)
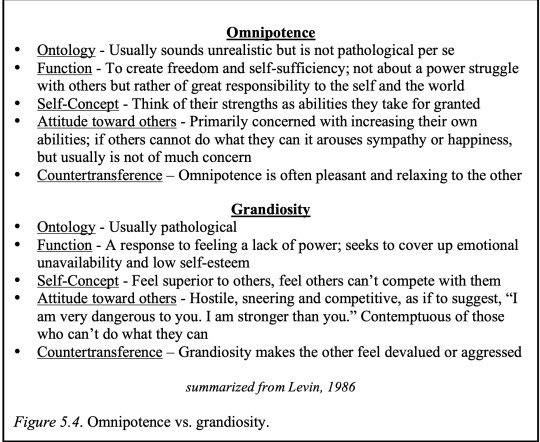
Schizoid omnipotence is not the same as the grandiosity observed in narcissistic personalities, and has several distinguishing features. Levin (1986) notes some of the main differences, as summarized below. The function of omnipotence is to create freedom and self-sufficiency and reflects the assuming of responsibility for the self. As such, omnipotent people are primarily concerned with increasing their own abilities rather than being in competition with others (Levin, 1986). If others cannot do what they can it may arouse sympathy or happiness, but usually is not an occupying concern. In contrast, grandiosity is a response to feeling a lack of power and often reflects an effort to cover up emotional unavailability and low self-esteem. Grandiose patients feel superior to others, feel others can’t compete with them, and are aggressive and contemptuous of those who cant do what they can (Levin, 1986).
The formation of omnipotence in the schizoid is secondary to the identification with idealized parent figures created in lieu of their actual parents. The fantasized fusion between the good self and the idealized inner parent creates the illusion of a secure attachment and blissful dependency on inner objects. The ecstatic states that result serve a critical defensive process against possible fragmentation and the acknowledgement of negative feelings toward the parents. The role reversal between their infantile true self and the internalized pseudo-adult self allows the schizoid to stave off feelings of weakness and helplessness (Seinfeld, 1991). In other words, omnipotence is used to overcome the limitations of the caregivers by falsely portraying the self as a perfect nurturing parent while denying the neglect and misattunement of his actual caregivers (Klein, 1946). The schizoid’s fear of committing to a new relationship in the real world reflects the need to keep this fantasy in place. Because no man or woman can equal up to the idealized figures of his fantasy life, the schizoid has a rationale for staying single and unattached.