Fight-or-flight response is altered in healthy young people who had COVID-19
New research published in The Journal of Physiology found that otherwise healthy young people diagnosed with COVID-19, regardless of their symptom severity, have problems with their nervous system when compared with healthy control subjects.
Specifically, the system which oversees the fight-or-flight response, the sympathetic nervous system, seems to be abnormal (overactive in some instances and underactive in others) in those recently diagnosed with COVID-19.
These results are especially important given the emerging evidence of symptoms like racing hearts being reported in conjunction with “long-COVID.”
The impact of this alteration in fight-or-flight response, especially if prolonged, means that many processes within the body could be disrupted or affected. This research team has specifically been looking at the impact on the cardiovascular system – including blood pressure and blood flow – but the sympathetic nervous system is also important in exercise responses, the digestive system, the immune function, and more.
Understanding what happens in the body shortly following diagnosis of COVID-19 is an important first step towards understanding the potential long-term consequences of contracting the disease.
Importantly, if similar disruption of the flight-or-fight response, like that found here in young individuals, is present in older adults following COVID-19 infection, there may be substantial adverse implications for cardiovascular health.
The researchers studied lung function, exercise capacity, vascular function, and neural cardiovascular control (the control of heartbeat by the brain).
They used a technique called microneurography, wherein the researchers inserted a tiny needle with an electrode into a nerve behind the knee, which records the electrical impulses of that nerve and measures how many bursts of electrical activity are happening and how big the bursts are.
From this nerve activity, they can assess the function of the sympathetic nervous system through a series of tests. For all the tests, the subject was lying on their back on a bed. First, the researchers looked at the baseline resting activity of the nerves, heart rate, and blood pressure. Resting sympathetic nerve activity was higher in the COVID-19 participants than healthy people used as controls in the experiment.
Then, the subject did a “cold pressor test,” where they stick their hand in an ice-water mixture (~0° C) for two minutes. In healthy individuals, this causes a profound increase in that sympathetic nerve (fight-or-flight) activity and blood pressure. The COVID-19 subjects rated their pain substantially lower than healthy subjects typically do.
Finally, the participant was moved to an upright position (the bed they’re lying on can tilt up and down) to see how well their body can respond to a change in position. The COVID-19 subjects had a pretty large increase in heart rate during this test; they also had higher sympathetic nerve activity throughout the tilt test compared with other healthy young adults.
As with all research on humans, there are limitations to this study. However, the biggest limitation in the present study is its cross-sectional nature – in other words, we do not know what the COVID-19 subjects’ nervous system activity “looked like” before they were diagnosed with COVID-19.
These findings are consistent with the increasing reports of long-COVID symptoms pertaining to problems with the fight-or-flight response.
Abigail Stickford, senior author on this study said, “Through our collaborative project, we have been following this cohort of COVID-19 subjects for 6 months following their positive test results. This work was representative of short-term data, so the next steps for us are to wrap up data collection and interpret how the subjects have changed over this time.”
Reblogging this comic again as my other one is going around again. I think that this one deserves to be seen, too. Thousands of people have responded to my long COVID story and shared their experiences with long COVID. I wish you could read all of them, but I’ve summarized some of it here.
Millions of people continue to suffer from exhaustion, cognitive problems and other long-lasting symptoms after a coronavirus infection. The exact causes of the illness, known as long Covid, are not known. But new research offers clues, describing the toll the illness takes on the body and why it can be so debilitating.
Diagnosing Long Covid
Patients with severe Covid may wind up in hospitals or on ventilators until their symptoms resolve. Damage to the body from severe Covid — pneumonia, low oxygen, inflammation — typically shows up on traditional diagnostic tests.
Long Covid is different: A chronic illness with a wide variety of symptoms, many of which are not explainable using conventional lab tests. Difficulties in detecting the illness have led some doctors to dismiss patients, or to misdiagnose their symptoms as psychosomatic. But researchers looking more deeply at long Covid patients have found visible dysfunction throughout the body.
Studies estimate that perhaps 10 to 30 percent of people infected with the coronavirus may develop long-term symptoms. It’s unclear why some people develop long Covid and others don’t, but four factors appear to increase the risk: high levels of viral RNA early during an infection, the presence of certain autoantibodies, the reactivation of Epstein-Barr virus and having Type 2 diabetes.
The Immune System
“Dang, why am I always so sick?”— Messiah Rodriguez, 17
Long Covid patients appear to have disruptedimmune systems compared to post-Covid patients who fully recover. Many researchers believe chronic immune dysfunction after a coronavirus infection may set off a chain of symptoms throughout the body.
One possibility is that the body is still fighting remnants of the coronavirus. Researchers found that the virus spreads widely during an initial infection, and that viral genetic material can remain embedded in tissues — in the intestines, lymph nodes and elsewhere — for many months.
Figure: Coronavirus RNA is visible in different body tissues at 500x magnification. Daniel Chertow et al., preprint via Research Square
Ongoing studies are trying to determine if these viral reservoirs cause inflammation in surrounding tissues, which could lead to brain fog, gastrointestinal problems and other symptoms.
Figure: Coronavirus components persist in one patient’s small intestine, 92 days after the start of their Covid symptoms. Christian Gaebler et al., Nature
Researchers have also found evidence that Covid may trigger a lasting and damaging autoimmune response. Studies have found surprisingly high levels of autoantibodies, which mistakenly attack a patient’s own tissues, many months after an initial infection.
A third possibility is that the initial viral infection triggers chronic inflammation, possibly by reactivating other viruses in the patient’s body that are normally dormant. The reactivation of Epstein-Barr virus, which infects most people when they are young, might help predict whether a person will develop long Covid, one study found.
Inside the intricate world of the immune system, these explanations may coexist. And just as different long Covid patients may have different symptoms, they may also have different immune problems, too. Identifying the problems that are central to each patient’s illness will be critical for guiding treatment, said Dr. Akiko Iwasaki, an immunologist at Yale.
For instance, a patient with autoantibodies might benefit from immunosuppressive medication, while a patient with remnants of the Covid virus should receive antivirals, Dr. Iwasaki said. “Depending on what each person has, the treatment would be quite different.”
The Circulatory System
“Something as simple as climbing on a ladder all of a sudden became a mountain.”— Eddie Palacios, 50
Many long Covid patients struggle with physical activity long after their initial infection, and experience a relapse of symptoms if they exercise. Initial studies suggest that dysfunction in the circulatory system might impair the flow of oxygen to muscles and other tissues, limiting aerobic capacity and causing severe fatigue.
Inone study, patients with long-lasting Covid symptoms had unexpected responses to riding a bike. Despite having apparently normal hearts and lungs, their muscles were only able to extract a portion of the normal amount of oxygen from small blood vessels as they pedaled, markedly reducing their exercise capacity.
One possible culprit: Chronic inflammation may damage nerve fibers that help control circulation, a condition called small fiber neuropathy. The damaged fibers, seen in skin biopsies, are associated with dysautonomia, a malfunction of automatic functions like heart rate, breathing and digestion that is very common in long Covid patients.
Figure: Chronic inflammation in long Covid patients may damage small nerve fibers. Peter Novak et al., Annals of Neurology
These findings demonstrate that people with long Covid are suffering systemic physical problems, rather than just being anxious or out of shape, said Dr. David M. Systrom, an exercise physiologist at Brigham and Women’s Hospital who helped conduct the bike study.
“You can’t make up small fiber neuropathy by skin biopsy. That isn’t in somebody’s head,” Dr. Systrom said. “You can’t make up poor oxygen extraction to this degree. All of these are objective measures of disease.”
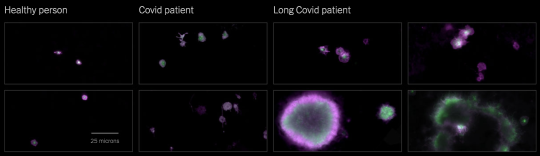
South African researchers found another circulation problem: Microscopic blood clots. Tiny clots that form during an initial Covid infection will typically break down naturally, but might persist in long Covid patients. These clots could block the tiny capillaries that carry oxygen to tissues throughout the body.
Figure: Platelets in the blood can become hyperactivated in Covid and long Covid patients, contributing to microclots. Etheresia Pretorius et al., Cardiovascular Diabetology
Inflammatory substances called cytokines, which are often elevated in long Covid patients, may injure the mitochondria that power the body’s cells, making them less able to use oxygen. Walls of blood vessels may also become inflamed, limiting the uptake of oxygen.
Whatever the cause, low oxygen levels may contribute to long Covid’s most common symptom, severe fatigue. Some long Covid patients meet the criteria for ME/CFS (also known as chronic fatigue syndrome), which often starts after a viral infection. Researchers have found that ME/CFS patients also suffer from a lack of oxygen triggered by circulatory problems. That puts enormous strain on the body’s metabolism and makes simple activities feel like strenuous exercise.
The Brain
“I approach a red light, my brain knows that it’s red, but it’s not reacting to the rest of my body to put my foot on the brake. Do you understand how terrifying that is?”— Samantha Lewis, 34
Even people with mild cases of Covid can experience sustained cognitive impairments, including reduced attention, memory and word-finding. Possible long-term neurological problems from Covid constitute “a major public health crisis,” according to Dr. Avindra Nath, the clinical director of the National Institute of Neurological Disorders and Stroke.
Researchers found a wide range of dysfunction in the brains of long Covid patients. Although it is unclear how often the virus directly penetrates the brain, even mild infections appear to cause significant brain inflammation, according to the researchers, who included Dr. Nath, Dr. Iwasaki and Dr. Michelle Monje, a neurologist at Stanford.
Infections may trigger the over-activation of immune cells called microglia in a way that appears similar to the process that can contribute to cognitive problems in aging and some neurodegenerative diseases.
Figure: Microglia are activated in the brain of a Covid patient, contributing to brain inflammation. Anthony Fernández-Castañeda et al., preprint via bioRxiv. Photos: Myoung-Hwa Lee
Another research group found that long Covid may significantly reduce the amount of blood that reaches the brain, a finding that has was also seen in patients with a related chronic condition, ME/CFS, before the pandemic.
The Lungs
“I couldn’t breathe. It literally felt like someone was sitting on my chest.”— Angelica Baez, 23
Shortness of breath is a frequent symptom of long Covid. But common lung tests — including chest X-rays, CT scans and functional tests — often come back normal.
Using specialized M.R.I. scans, a team of British researchers found preliminary evidence of lung damage in a small group of long Covid patients who had never been hospitalized. Detailed scans of their lung function indicated that most of the patients took up oxygen less efficiently than healthy people did, even if the structure of their lungs appeared to be normal.
The researchers cautioned that a larger group of patients will be needed to confirm the findings. If the results hold up, possible explanations for the observed shortness of breath include microclots in lung tissues or a thickening of the blood-air barrier that regulates the uptake of oxygen in the lungs.
Living With Long Covid
“It’s really not something you can push through.”— Dr. Abigail Bosk
Many hospitals now offer post-Covid clinics or recovery programs, which bring together doctors with experience treating long Covid patients. Given the number of patients, some doctors and programs have long waits for appointments. It can help to plan ahead and try multiple options.
— Americans with long Covid may qualify for disability benefits, although without conclusive medical results, many people face roadblocks.
— Three leading researchers into long Covid often share information about the latest findings on Twitter: Dr. Amy Proal, a microbiologist at PolyBio Research Institute; Dr. David Putrino, the director of rehabilitation innovation for the Mount Sinai Health System; and Dr. Iwasaki, the Yale immunologist.
—Health Rising covers the latest research into long Covid, ME/CFS and other chronic illnesses in detail.
— Gez Medinger, a video producer, interviews some prominent researchers into long Covid on YouTube.
— A video interview with Dr. Svetlana Blitshteyn, a neurologist and the director of the Dysautonomia Clinic, offers advice for treatment and an overview of current research into autonomic disorders.
— A detailed guide to understanding, treating and living with orthostatic intolerance is available from the Johns Hopkins Children’s Center.
Source: by Josh Keller(The New York Times). Illustration by Violet Frances for Bryan Christie Design. Produced by Jonathan Corum. Additional reporting by Pam Belluck and Amanda Morris.
Long COVID isn’t going away, and we still do not have a way to fully prevent it, cure it, or really to quantify it.
The world was slow to recognize long COVID as one of the most serious consequences of the coronavirus. Six months into the pathogen’s tear across the globe, SARS-CoV-2 was still considered an acute airway infection that would spark a weeks-long illness at most; anyone who experienced symptoms for longer could be expected to be dismissed by droves of doctors. Now long COVID is written into CDC and WHO documents; it makes a cameo in the newest version of President Joe Biden’s National COVID-19 Preparedness Plan.
But for all we knownowabout long COVID, it is still not enough. Researchers still don’t know who’s most at risk, or how long the condition might last; whether certain variants might cause it more frequently, or the extent to which vaccines might sweep it away. We do not have a way to fully prevent it. We do not have a way to cure it. We don’t even have a way to really quantify it: There still isn’t consensus on how common long COVID actually is. Its danger feels both amorphous and unavoidable. People already struggle to deal with well-known risks, let alone fuzzy, slippery ones. “You can be too afraid of what you don’t understand or just say, ‘It’s not well defined; I’m not going to think about it,’” says Erin Sanders, a nurse practitioner and clinical scientist at MIT. Concern, when we let it, can act like a gas. It expands to fill the space we give it.
But even if long COVID’s prevalence turns out to be a single-digit percentage of SARS-CoV-2 infections—proportionally much smaller than most experts estimate—in absolute terms “that is not small,” says Ziyad Al-Aly, the director of the Clinical Epidemiology Center at the Veterans Affairs St. Louis Health Care System. Millions of people have already developed long COVID; many of them, an untold fraction, have not recovered. This is the challenge of chronic illness: When people join its ranks, they do not always exit. With each new case of long COVID, the virus’s burden balloons.
“I worry, now that everyone is moving to the post-pandemic world, we’re going to sweep all these patients under the rug,” Al-Aly said. Long COVID struggled to gain a toehold in the national consciousness; now it threatens to be one of the first major COVID impacts to slip back into the margins.
Researchers have known for many months that long COVID is more a category than a monolith. Al-Aly very roughly likens it to the way we talk about cancer—an umbrella term for diseases that are related but that require distinct diagnoses and treatments. Long COVID has hundreds of possible symptoms. It can batter the brain, the heart, the lungs, the gut, all of the above, or none of the above. The condition can start from a silent infection, an ICU-caliber case, or anything in between. It can begin days, weeks, or months after the virus first infects someone, and its severity can fluctuate over time. “We lump all of that into one broad thing,” Al-Aly said. “It is not.”
The condition’s root causes, accordingly, are also diverse. In some cases, long COVID may be collateral damage from the war waged between virus and immune system; in others, it might sprout out of a chronic SARS-CoV-2 infection or, conversely, a quick viral encounter that sets bodily systems on the fritz. These hypotheses aren’t comprehensive or mutually exclusive: There are only so many ways for bodies to run smoothly, and infinite ways to throw those processes out of whack.
All of this means that even diagnosing long COVID—an essential step toward understanding it—is still a battle. We don’t have a clear-cut, consensus clinical definition, a single name for the condition, or a standardized set of tests to catch it. Even the CDC and the WHO can’t agree on how long a person must be sick before they meet the condition’s criteria. Some researchers and health-care providers favor one agency’s definition; others, dissatisfied with both, come up with their own. And “there are still doctors out there that do not think long COVID exists,” says Alexandra Yonts, a pediatric-infectious-disease specialist at Children’s National Hospital, in Washington, D.C.
In an ideal experimental world, to understand long COVID’s risks, researchers would systematically survey large swaths of the population over long periods of time, watching to see who gets infected, who goes on to develop the condition, what form it takes, and how it impacts people’s health, says Shruti Mehta, an infectious-disease epidemiologist at the Johns Hopkins Bloomberg School of Public Health who is studying long COVID. But few institutions have the resources for such an undertaking, which could span many months or years. So many researchers have to make do with the limited data sets that are already available to them. As a result, some studies end up biased toward patients who were hospitalized, while others wind up favoring people who have the time, means, and trust in the health-care system to sign up for long-term studies. Neither group fully captures long COVID’s wide-ranging toll. The situation’s especially tough for pediatric patients, who might be too young to articulate the severity of their symptoms and are often excluded from long-COVID studies. Long COVID certainly exists in kids, but it may not perfectly mirror what goes on in adults: Children’s susceptibility to the virus is different, and their bodies are so rapidly changing, says Yonts, who runs a pediatric-long-COVID clinic in D.C.
All told, the study of long COVID has become, as Sanders of MIT puts it, “a data disaster.” Some researchers estimate that a single-digit percentage of SARS-CoV-2 infections bloom into long COVID; Al-Aly is one of them. Others, meanwhile, favor larger numbers, with a few even insisting that the rates are actually more than half. Most of the experts said they feel comfortable working in the 10 to30 percent range, which is where many studies seem to be starting to converge. Finding one answer is tricky, without knowing how many forms long COVID can take—some could be more common than others. Formally splitting the disease into subdivisions could help address some of these ambiguities. But we don’t know nearly enough to start slicing and dicing, says Bryan Lau, an infectious-disease epidemiologist working with Mehta and Priya Duggal.
If researchers aren’t comprehensively capturing who currently has long COVID, they can’t say for certain who’s most likely to get it either. Manyresearchershavefound that women contract long COVID more frequently than men. Others have uncovered evidence that people who end up infected with gobs of the coronavirus, or who produce antibodies that attack the body’s own tissues, also seem to tilt toward long COVID. Chronic health issues, including diabetes, could up a person’s chances of getting sick and staying sick as well. So might a lingering Epstein-Barr virus infection. But some of these trends are still being confirmed, experts said, and the extent to which they toggle risk up or down isn’t known. And it’s definitely too early to pinpoint any of these factors as long-COVID causes. “For acute COVID, we know what the risk factors are,” Akiko Iwasaki, an immunologist studying long COVID at Yale, said. “For long COVID, it’s much less clear.”
Still, a couple of other variables feel a bit more nailed down. “The riskishigh in people who need hospitalization or ICU care,” Al-Aly said. Deepti Gurdasani, an epidemiologist at Queen Mary University of London, says she’s fairly confident that the nature of a person’s exposure to SARS-CoV-2 plays a role as well: Heavier and more frequent viral encounters seem to tip the scales toward symptoms that last and last. That’s a concern for people in essential occupations, who “aren’t able to shield themselves,” she said.
If these last few factors directly affect how and whether long COVID unspools, vaccination—which reliably staves off hospitalization and, to a lesser degree, infection—could be a partial preventive. Severalstudies have shown that shots do seem to muzzle long-COVID rates. They don’t, however, eliminate long COVID’s odds. To date, experts have yet to find any demographic that has been spared from the condition, despite persistent myths that certain groups, particularly kids, are somehow immune. “We’ve seen it in children of all ages,” says Laura Malone, a pediatric neurologist at the Kennedy Krieger Institute, in Baltimore. Some of her patients are toddlers. The virus isn’t pulling any punches either. Every iteration we’ve encountered so far, Omicron included, seems capable of causing long COVID. “No one is not at risk,” Al-Aly said.
To this day, most countries do not keep a running tally of long-COVID cases. But ballparks of the burden are staggering. Some 2 percent of all U.K. residents—not just those with documented infections—might currently have long COVID, according to the Office for National Statistics. Another analysis estimates that up to 23 million Americans have developed the condition since the pandemic’s start. More will join them. But Davis worries that those numbers will continue to be left off of national dashboards, and thus out of the public eye. Now that the federal government has tightened the boundaries of its concern to hospitalizations and deaths, the public does not even really have to look away from the national perspective on long COVID: There is next to nothing to see.
As people rack up different combinations of shots and infections with different variants, what worsens or soothes long COVID is also getting harder to understand. Many of the experts think long COVID is essential to study, it’s too complex for them to want to tackle themselves. Meanwhile, long COVID remains the pandemic’s looming specter. We are told there is risk, but not exactly how much; we are told that avoiding long COVID would be ideal, but lack the practical guidance to do so—the virus is so widespread that eventual infection, for many people, feels almost inevitable.
At the same time, as researchers look deeper and deeper into the bodies of infected people, they’re only seeing more damage. With each passing month, more studies emerge documenting how the coronavirus alters the function of vital organs such as the heart and the brain. The public has been cultured to think that most SARS-CoV-2 infections are trivial, and the repercussions brief, especially for the young, healthy, and privileged. But long COVID breaks the binary of severe and mild. “It’s going to continue to affect people, even people who are protected from severe illness during the acute phase of infection,” Michael Peluso, an infectious-disease physician and long-COVID researcher at UC San Francisco, said.
No matter where the true numbers on long-COVID risk sit, they are too large to ignore. “Whether it’s 10 percent or 50 percent, at both levels you have to do something about it,” Gurdasani said. Statistics will help sharpen and clarify the condition’s boundaries, and are still worth seeking out. They will not, however, change long COVID’s threat, at its core.
Davis, who is nearing her second anniversary of developing long COVID, feels this deeply. She is still experiencing cognitive dysfunction and memory loss. Her heart still races when she stands. “You cannot live your life like you used to,” she said. “Your life just becomes this shell.” For individuals, for societies, “this is not going away.” Even after much of the world puts the pandemic in its rearview, long COVID will keep filling hospitals and clinics. It will dot the pages of scientific texts, and linginfer in the bodies of millions of people worldwide. Hospitalizations and ICU admissions are not the only COVID outcomes that can buckle a health-care system.
That strain is already being felt by the health-care workers on long COVID’s front lines. Yonts, the Children’s National pediatrician, said that she’s currently booking patients “out to Memorial Day.” COVID’s global crisis can, in some ways, end when we decide to treat it as done. But that is not an option for a growing fraction of the planet, who cannot put COVID fully behind them. “This is going to be the pandemic after the pandemic,” Gurdasani said.
it supports a body of evidence she’s been gathering over decadesthat indicates that many more people might be at risk of serious health complications from infections than our available data gathering methods can detect - and that dysfunction in the immune system, pre-existing or not, might play some role in post-acute infectious syndromes.
If a lot more funding has been given to ME and fibromyalgia research and if these conditions and the patients had actually been taken seriously and not made out to be “in our heads” I believe we’d be a lot closer to figuring out long covid right now and there would be more available to support the masses of people who have developed this awful chronic illness
Millions of people continue to suffer from exhaustion, cognitive problems and other long-lasting symptoms after a coronavirus infection. The exact causes of the illness, known as long Covid, are not known. But new research offers clues, describing the toll the illness takes on the body and why it can be so debilitating.
Diagnosing Long Covid
Patients with severe Covid may wind up in hospitals or on ventilators until their symptoms resolve. Damage to the body from severe Covid — pneumonia, low oxygen, inflammation — typically shows up on traditional diagnostic tests.
Long Covid is different: A chronic illness with a wide variety of symptoms, many of which are not explainable using conventional lab tests. Difficulties in detecting the illness have led some doctors to dismiss patients, or to misdiagnose their symptoms as psychosomatic. But researchers looking more deeply at long Covid patients have found visible dysfunction throughout the body.
Studies estimate that perhaps 10 to 30 percent of people infected with the coronavirus may develop long-term symptoms. It’s unclear why some people develop long Covid and others don’t, but four factors appear to increase the risk: high levels of viral RNA early during an infection, the presence of certain autoantibodies, the reactivation of Epstein-Barr virus and having Type 2 diabetes.
The Immune System
“Dang, why am I always so sick?”— Messiah Rodriguez, 17
Long Covid patients appear to have disruptedimmune systems compared to post-Covid patients who fully recover. Many researchers believe chronic immune dysfunction after a coronavirus infection may set off a chain of symptoms throughout the body.
One possibility is that the body is still fighting remnants of the coronavirus. Researchers found that the virus spreads widely during an initial infection, and that viral genetic material can remain embedded in tissues — in the intestines, lymph nodes and elsewhere — for many months.
Figure: Coronavirus RNA is visible in different body tissues at 500x magnification. Daniel Chertow et al., preprint via Research Square
Ongoing studies are trying to determine if these viral reservoirs cause inflammation in surrounding tissues, which could lead to brain fog, gastrointestinal problems and other symptoms.
Figure: Coronavirus components persist in one patient’s small intestine, 92 days after the start of their Covid symptoms. Christian Gaebler et al., Nature
Researchers have also found evidence that Covid may trigger a lasting and damaging autoimmune response. Studies have found surprisingly high levels of autoantibodies, which mistakenly attack a patient’s own tissues, many months after an initial infection.
A third possibility is that the initial viral infection triggers chronic inflammation, possibly by reactivating other viruses in the patient’s body that are normally dormant. The reactivation of Epstein-Barr virus, which infects most people when they are young, might help predict whether a person will develop long Covid, one study found.
Inside the intricate world of the immune system, these explanations may coexist. And just as different long Covid patients may have different symptoms, they may also have different immune problems, too. Identifying the problems that are central to each patient’s illness will be critical for guiding treatment, said Dr. Akiko Iwasaki, an immunologist at Yale.
For instance, a patient with autoantibodies might benefit from immunosuppressive medication, while a patient with remnants of the Covid virus should receive antivirals, Dr. Iwasaki said. “Depending on what each person has, the treatment would be quite different.”
The Circulatory System
“Something as simple as climbing on a ladder all of a sudden became a mountain.”— Eddie Palacios, 50
Many long Covid patients struggle with physical activity long after their initial infection, and experience a relapse of symptoms if they exercise. Initial studies suggest that dysfunction in the circulatory system might impair the flow of oxygen to muscles and other tissues, limiting aerobic capacity and causing severe fatigue.
Inone study, patients with long-lasting Covid symptoms had unexpected responses to riding a bike. Despite having apparently normal hearts and lungs, their muscles were only able to extract a portion of the normal amount of oxygen from small blood vessels as they pedaled, markedly reducing their exercise capacity.
One possible culprit: Chronic inflammation may damage nerve fibers that help control circulation, a condition called small fiber neuropathy. The damaged fibers, seen in skin biopsies, are associated with dysautonomia, a malfunction of automatic functions like heart rate, breathing and digestion that is very common in long Covid patients.
Figure: Chronic inflammation in long Covid patients may damage small nerve fibers. Peter Novak et al., Annals of Neurology
These findings demonstrate that people with long Covid are suffering systemic physical problems, rather than just being anxious or out of shape, said Dr. David M. Systrom, an exercise physiologist at Brigham and Women’s Hospital who helped conduct the bike study.
“You can’t make up small fiber neuropathy by skin biopsy. That isn’t in somebody’s head,” Dr. Systrom said. “You can’t make up poor oxygen extraction to this degree. All of these are objective measures of disease.”
South African researchers found another circulation problem: Microscopic blood clots. Tiny clots that form during an initial Covid infection will typically break down naturally, but might persist in long Covid patients. These clots could block the tiny capillaries that carry oxygen to tissues throughout the body.
Figure: Platelets in the blood can become hyperactivated in Covid and long Covid patients, contributing to microclots. Etheresia Pretorius et al., Cardiovascular Diabetology
Inflammatory substances called cytokines, which are often elevated in long Covid patients, may injure the mitochondria that power the body’s cells, making them less able to use oxygen. Walls of blood vessels may also become inflamed, limiting the uptake of oxygen.
Whatever the cause, low oxygen levels may contribute to long Covid’s most common symptom, severe fatigue. Some long Covid patients meet the criteria for ME/CFS (also known as chronic fatigue syndrome), which often starts after a viral infection. Researchers have found that ME/CFS patients also suffer from a lack of oxygen triggered by circulatory problems. That puts enormous strain on the body’s metabolism and makes simple activities feel like strenuous exercise.
The Brain
“I approach a red light, my brain knows that it’s red, but it’s not reacting to the rest of my body to put my foot on the brake. Do you understand how terrifying that is?”— Samantha Lewis, 34
Even people with mild cases of Covid can experience sustained cognitive impairments, including reduced attention, memory and word-finding. Possible long-term neurological problems from Covid constitute “a major public health crisis,” according to Dr. Avindra Nath, the clinical director of the National Institute of Neurological Disorders and Stroke.
Researchers found a wide range of dysfunction in the brains of long Covid patients. Although it is unclear how often the virus directly penetrates the brain, even mild infections appear to cause significant brain inflammation, according to the researchers, who included Dr. Nath, Dr. Iwasaki and Dr. Michelle Monje, a neurologist at Stanford.
Infections may trigger the over-activation of immune cells called microglia in a way that appears similar to the process that can contribute to cognitive problems in aging and some neurodegenerative diseases.
Figure: Microglia are activated in the brain of a Covid patient, contributing to brain inflammation. Anthony Fernández-Castañeda et al., preprint via bioRxiv. Photos: Myoung-Hwa Lee
Another research group found that long Covid may significantly reduce the amount of blood that reaches the brain, a finding that has was also seen in patients with a related chronic condition, ME/CFS, before the pandemic.
The Lungs
“I couldn’t breathe. It literally felt like someone was sitting on my chest.”— Angelica Baez, 23
Shortness of breath is a frequent symptom of long Covid. But common lung tests — including chest X-rays, CT scans and functional tests — often come back normal.
Using specialized M.R.I. scans, a team of British researchers found preliminary evidence of lung damage in a small group of long Covid patients who had never been hospitalized. Detailed scans of their lung function indicated that most of the patients took up oxygen less efficiently than healthy people did, even if the structure of their lungs appeared to be normal.
The researchers cautioned that a larger group of patients will be needed to confirm the findings. If the results hold up, possible explanations for the observed shortness of breath include microclots in lung tissues or a thickening of the blood-air barrier that regulates the uptake of oxygen in the lungs.
Living With Long Covid
“It’s really not something you can push through.”— Dr. Abigail Bosk
Many hospitals now offer post-Covid clinics or recovery programs, which bring together doctors with experience treating long Covid patients. Given the number of patients, some doctors and programs have long waits for appointments. It can help to plan ahead and try multiple options.
— Americans with long Covid may qualify for disability benefits, although without conclusive medical results, many people face roadblocks.
— Three leading researchers into long Covid often share information about the latest findings on Twitter: Dr. Amy Proal, a microbiologist at PolyBio Research Institute; Dr. David Putrino, the director of rehabilitation innovation for the Mount Sinai Health System; and Dr. Iwasaki, the Yale immunologist.
—Health Rising covers the latest research into long Covid, ME/CFS and other chronic illnesses in detail.
— Gez Medinger, a video producer, interviews some prominent researchers into long Covid on YouTube.
— A video interview with Dr. Svetlana Blitshteyn, a neurologist and the director of the Dysautonomia Clinic, offers advice for treatment and an overview of current research into autonomic disorders.
— A detailed guide to understanding, treating and living with orthostatic intolerance is available from the Johns Hopkins Children’s Center.
Source: by Josh Keller(The New York Times). Illustration by Violet Frances for Bryan Christie Design. Produced by Jonathan Corum. Additional reporting by Pam Belluck and Amanda Morris.
Long COVID isn’t going away, and we still do not have a way to fully prevent it, cure it, or really to quantify it.
The world was slow to recognize long COVID as one of the most serious consequences of the coronavirus. Six months into the pathogen’s tear across the globe, SARS-CoV-2 was still considered an acute airway infection that would spark a weeks-long illness at most; anyone who experienced symptoms for longer could be expected to be dismissed by droves of doctors. Now long COVID is written into CDC and WHO documents; it makes a cameo in the newest version of President Joe Biden’s National COVID-19 Preparedness Plan.
But for all we knownowabout long COVID, it is still not enough. Researchers still don’t know who’s most at risk, or how long the condition might last; whether certain variants might cause it more frequently, or the extent to which vaccines might sweep it away. We do not have a way to fully prevent it. We do not have a way to cure it. We don’t even have a way to really quantify it: There still isn’t consensus on how common long COVID actually is. Its danger feels both amorphous and unavoidable. People already struggle to deal with well-known risks, let alone fuzzy, slippery ones. “You can be too afraid of what you don’t understand or just say, ‘It’s not well defined; I’m not going to think about it,’” says Erin Sanders, a nurse practitioner and clinical scientist at MIT. Concern, when we let it, can act like a gas. It expands to fill the space we give it.
But even if long COVID’s prevalence turns out to be a single-digit percentage of SARS-CoV-2 infections—proportionally much smaller than most experts estimate—in absolute terms “that is not small,” says Ziyad Al-Aly, the director of the Clinical Epidemiology Center at the Veterans Affairs St. Louis Health Care System. Millions of people have already developed long COVID; many of them, an untold fraction, have not recovered. This is the challenge of chronic illness: When people join its ranks, they do not always exit. With each new case of long COVID, the virus’s burden balloons.
“I worry, now that everyone is moving to the post-pandemic world, we’re going to sweep all these patients under the rug,” Al-Aly said. Long COVID struggled to gain a toehold in the national consciousness; now it threatens to be one of the first major COVID impacts to slip back into the margins.
Researchers have known for many months that long COVID is more a category than a monolith. Al-Aly very roughly likens it to the way we talk about cancer—an umbrella term for diseases that are related but that require distinct diagnoses and treatments. Long COVID has hundreds of possible symptoms. It can batter the brain, the heart, the lungs, the gut, all of the above, or none of the above. The condition can start from a silent infection, an ICU-caliber case, or anything in between. It can begin days, weeks, or months after the virus first infects someone, and its severity can fluctuate over time. “We lump all of that into one broad thing,” Al-Aly said. “It is not.”
The condition’s root causes, accordingly, are also diverse. In some cases, long COVID may be collateral damage from the war waged between virus and immune system; in others, it might sprout out of a chronic SARS-CoV-2 infection or, conversely, a quick viral encounter that sets bodily systems on the fritz. These hypotheses aren’t comprehensive or mutually exclusive: There are only so many ways for bodies to run smoothly, and infinite ways to throw those processes out of whack.
All of this means that even diagnosing long COVID—an essential step toward understanding it—is still a battle. We don’t have a clear-cut, consensus clinical definition, a single name for the condition, or a standardized set of tests to catch it. Even the CDC and the WHO can’t agree on how long a person must be sick before they meet the condition’s criteria. Some researchers and health-care providers favor one agency’s definition; others, dissatisfied with both, come up with their own. And “there are still doctors out there that do not think long COVID exists,” says Alexandra Yonts, a pediatric-infectious-disease specialist at Children’s National Hospital, in Washington, D.C.
In an ideal experimental world, to understand long COVID’s risks, researchers would systematically survey large swaths of the population over long periods of time, watching to see who gets infected, who goes on to develop the condition, what form it takes, and how it impacts people’s health, says Shruti Mehta, an infectious-disease epidemiologist at the Johns Hopkins Bloomberg School of Public Health who is studying long COVID. But few institutions have the resources for such an undertaking, which could span many months or years. So many researchers have to make do with the limited data sets that are already available to them. As a result, some studies end up biased toward patients who were hospitalized, while others wind up favoring people who have the time, means, and trust in the health-care system to sign up for long-term studies. Neither group fully captures long COVID’s wide-ranging toll. The situation’s especially tough for pediatric patients, who might be too young to articulate the severity of their symptoms and are often excluded from long-COVID studies. Long COVID certainly exists in kids, but it may not perfectly mirror what goes on in adults: Children’s susceptibility to the virus is different, and their bodies are so rapidly changing, says Yonts, who runs a pediatric-long-COVID clinic in D.C.
All told, the study of long COVID has become, as Sanders of MIT puts it, “a data disaster.” Some researchers estimate that a single-digit percentage of SARS-CoV-2 infections bloom into long COVID; Al-Aly is one of them. Others, meanwhile, favor larger numbers, with a few even insisting that the rates are actually more than half. Most of the experts said they feel comfortable working in the 10 to30 percent range, which is where many studies seem to be starting to converge. Finding one answer is tricky, without knowing how many forms long COVID can take—some could be more common than others. Formally splitting the disease into subdivisions could help address some of these ambiguities. But we don’t know nearly enough to start slicing and dicing, says Bryan Lau, an infectious-disease epidemiologist working with Mehta and Priya Duggal.
If researchers aren’t comprehensively capturing who currently has long COVID, they can’t say for certain who’s most likely to get it either. Manyresearchershavefound that women contract long COVID more frequently than men. Others have uncovered evidence that people who end up infected with gobs of the coronavirus, or who produce antibodies that attack the body’s own tissues, also seem to tilt toward long COVID. Chronic health issues, including diabetes, could up a person’s chances of getting sick and staying sick as well. So might a lingering Epstein-Barr virus infection. But some of these trends are still being confirmed, experts said, and the extent to which they toggle risk up or down isn’t known. And it’s definitely too early to pinpoint any of these factors as long-COVID causes. “For acute COVID, we know what the risk factors are,” Akiko Iwasaki, an immunologist studying long COVID at Yale, said. “For long COVID, it’s much less clear.”
Still, a couple of other variables feel a bit more nailed down. “The riskishigh in people who need hospitalization or ICU care,” Al-Aly said. Deepti Gurdasani, an epidemiologist at Queen Mary University of London, says she’s fairly confident that the nature of a person’s exposure to SARS-CoV-2 plays a role as well: Heavier and more frequent viral encounters seem to tip the scales toward symptoms that last and last. That’s a concern for people in essential occupations, who “aren’t able to shield themselves,” she said.
If these last few factors directly affect how and whether long COVID unspools, vaccination—which reliably staves off hospitalization and, to a lesser degree, infection—could be a partial preventive. Severalstudies have shown that shots do seem to muzzle long-COVID rates. They don’t, however, eliminate long COVID’s odds. To date, experts have yet to find any demographic that has been spared from the condition, despite persistent myths that certain groups, particularly kids, are somehow immune. “We’ve seen it in children of all ages,” says Laura Malone, a pediatric neurologist at the Kennedy Krieger Institute, in Baltimore. Some of her patients are toddlers. The virus isn’t pulling any punches either. Every iteration we’ve encountered so far, Omicron included, seems capable of causing long COVID. “No one is not at risk,” Al-Aly said.
To this day, most countries do not keep a running tally of long-COVID cases. But ballparks of the burden are staggering. Some 2 percent of all U.K. residents—not just those with documented infections—might currently have long COVID, according to the Office for National Statistics. Another analysis estimates that up to 23 million Americans have developed the condition since the pandemic’s start. More will join them. But Davis worries that those numbers will continue to be left off of national dashboards, and thus out of the public eye. Now that the federal government has tightened the boundaries of its concern to hospitalizations and deaths, the public does not even really have to look away from the national perspective on long COVID: There is next to nothing to see.
As people rack up different combinations of shots and infections with different variants, what worsens or soothes long COVID is also getting harder to understand. Many of the experts think long COVID is essential to study, it’s too complex for them to want to tackle themselves. Meanwhile, long COVID remains the pandemic’s looming specter. We are told there is risk, but not exactly how much; we are told that avoiding long COVID would be ideal, but lack the practical guidance to do so—the virus is so widespread that eventual infection, for many people, feels almost inevitable.
At the same time, as researchers look deeper and deeper into the bodies of infected people, they’re only seeing more damage. With each passing month, more studies emerge documenting how the coronavirus alters the function of vital organs such as the heart and the brain. The public has been cultured to think that most SARS-CoV-2 infections are trivial, and the repercussions brief, especially for the young, healthy, and privileged. But long COVID breaks the binary of severe and mild. “It’s going to continue to affect people, even people who are protected from severe illness during the acute phase of infection,” Michael Peluso, an infectious-disease physician and long-COVID researcher at UC San Francisco, said.
No matter where the true numbers on long-COVID risk sit, they are too large to ignore. “Whether it’s 10 percent or 50 percent, at both levels you have to do something about it,” Gurdasani said. Statistics will help sharpen and clarify the condition’s boundaries, and are still worth seeking out. They will not, however, change long COVID’s threat, at its core.
Davis, who is nearing her second anniversary of developing long COVID, feels this deeply. She is still experiencing cognitive dysfunction and memory loss. Her heart still races when she stands. “You cannot live your life like you used to,” she said. “Your life just becomes this shell.” For individuals, for societies, “this is not going away.” Even after much of the world puts the pandemic in its rearview, long COVID will keep filling hospitals and clinics. It will dot the pages of scientific texts, and linginfer in the bodies of millions of people worldwide. Hospitalizations and ICU admissions are not the only COVID outcomes that can buckle a health-care system.
That strain is already being felt by the health-care workers on long COVID’s front lines. Yonts, the Children’s National pediatrician, said that she’s currently booking patients “out to Memorial Day.” COVID’s global crisis can, in some ways, end when we decide to treat it as done. But that is not an option for a growing fraction of the planet, who cannot put COVID fully behind them. “This is going to be the pandemic after the pandemic,” Gurdasani said.
Becoming chronically ill because of a virus or infection is such a surreal experience. One day, you were fine, and then after developing a simple cough, cold, or stomach flu, your life was changed forever.
One in five adult Covid survivors under the age of 65 in the United States has experienced at least one health condition that could be considered long Covid, according to a large new study by the Centers for Disease Control and Prevention. Among patients 65 and older, the number is even higher: one in four.
In an indication of how seriously the federal health agency views the problem of long Covid, the authors of the study — members of the C.D.C.’s Covid-19 Emergency Response Team — recommended “routine assessment for post-Covid conditions among persons who survive Covid-19.”
Long Covid is the term used to describe an array of symptoms that can last for months or longer after the initial coronavirus infection. The researchers identified post-Covid health problems in many different organ systems, including the heart, lungs and kidneys. Other issues involved blood circulation, the musculoskeletal system and the endocrine system; gastrointestinal conditions, neurological problems and psychiatric symptoms were also identified in the study.
trying in vain to blacklist all words related to smell cuz I’m two years and four months post covid and every single thing still smells and tastes like rotting meat and sewage and nothing is getting better and everyone else is living like everything is normal
I keep saying that the media only reporting death as THE negative result of getting covid has fucked up how we view catching this virus. Getting it, surviving but not being able to walk 2 blocks without passing out ain’t it.
Get your shots and wear a mask.
I recently got diagnosed with post-viral chronic fatigue syndrome & heart palpitations after suffering from other debilitating long COVID symptoms for two years. My ME/CFS is not as bad as this person’s, but I relate. I’m 21 and got COVID when I was 19 years old. I used to go to the gym 5 days a week. Not anymore!
Here’s a comic piece I did about my experience, and another comic about others’ long COVID experiences.
Thinking about how a year ago I was interviewed by a very popular radio show about my long COVID symptoms (I was over a year into experiencing them). They ended up not using my story because “it was too sad” and “I didn’t recover like other people”. They told me to contact them when I had recovered to potentially share my story in the future. I wrote back and told them that most people with long COVID will never recover, and that they weren’t accurately reporting on how COVID affects people. They never replied.
A year later and my symptoms still haven’t improved at all. Anyways, here’s your reminder that the COVID reporting you’re reading (at least in the U.S.) is probably not accurate and is not actually reflecting the suffering of real people.
Millions of people continue to suffer from exhaustion, cognitive problems and other long-lasting symptoms after a coronavirus infection. The exact causes of the illness, known as long Covid, are not known. But new research offers clues, describing the toll the illness takes on the body and why it can be so debilitating.
Diagnosing Long Covid
Patients with severe Covid may wind up in hospitals or on ventilators until their symptoms resolve. Damage to the body from severe Covid — pneumonia, low oxygen, inflammation — typically shows up on traditional diagnostic tests.
Long Covid is different: A chronic illness with a wide variety of symptoms, many of which are not explainable using conventional lab tests. Difficulties in detecting the illness have led some doctors to dismiss patients, or to misdiagnose their symptoms as psychosomatic. But researchers looking more deeply at long Covid patients have found visible dysfunction throughout the body.
Studies estimate that perhaps 10 to 30 percent of people infected with the coronavirus may develop long-term symptoms. It’s unclear why some people develop long Covid and others don’t, but four factors appear to increase the risk: high levels of viral RNA early during an infection, the presence of certain autoantibodies, the reactivation of Epstein-Barr virus and having Type 2 diabetes.
The Immune System
“Dang, why am I always so sick?”— Messiah Rodriguez, 17
Long Covid patients appear to have disruptedimmune systems compared to post-Covid patients who fully recover. Many researchers believe chronic immune dysfunction after a coronavirus infection may set off a chain of symptoms throughout the body.
One possibility is that the body is still fighting remnants of the coronavirus. Researchers found that the virus spreads widely during an initial infection, and that viral genetic material can remain embedded in tissues — in the intestines, lymph nodes and elsewhere — for many months.
Figure: Coronavirus RNA is visible in different body tissues at 500x magnification. Daniel Chertow et al., preprint via Research Square
Ongoing studies are trying to determine if these viral reservoirs cause inflammation in surrounding tissues, which could lead to brain fog, gastrointestinal problems and other symptoms.
Figure: Coronavirus components persist in one patient’s small intestine, 92 days after the start of their Covid symptoms. Christian Gaebler et al., Nature
Researchers have also found evidence that Covid may trigger a lasting and damaging autoimmune response. Studies have found surprisingly high levels of autoantibodies, which mistakenly attack a patient’s own tissues, many months after an initial infection.
A third possibility is that the initial viral infection triggers chronic inflammation, possibly by reactivating other viruses in the patient’s body that are normally dormant. The reactivation of Epstein-Barr virus, which infects most people when they are young, might help predict whether a person will develop long Covid, one study found.
Inside the intricate world of the immune system, these explanations may coexist. And just as different long Covid patients may have different symptoms, they may also have different immune problems, too. Identifying the problems that are central to each patient’s illness will be critical for guiding treatment, said Dr. Akiko Iwasaki, an immunologist at Yale.
For instance, a patient with autoantibodies might benefit from immunosuppressive medication, while a patient with remnants of the Covid virus should receive antivirals, Dr. Iwasaki said. “Depending on what each person has, the treatment would be quite different.”
The Circulatory System
“Something as simple as climbing on a ladder all of a sudden became a mountain.”— Eddie Palacios, 50
Many long Covid patients struggle with physical activity long after their initial infection, and experience a relapse of symptoms if they exercise. Initial studies suggest that dysfunction in the circulatory system might impair the flow of oxygen to muscles and other tissues, limiting aerobic capacity and causing severe fatigue.
Inone study, patients with long-lasting Covid symptoms had unexpected responses to riding a bike. Despite having apparently normal hearts and lungs, their muscles were only able to extract a portion of the normal amount of oxygen from small blood vessels as they pedaled, markedly reducing their exercise capacity.
One possible culprit: Chronic inflammation may damage nerve fibers that help control circulation, a condition called small fiber neuropathy. The damaged fibers, seen in skin biopsies, are associated with dysautonomia, a malfunction of automatic functions like heart rate, breathing and digestion that is very common in long Covid patients.
Figure: Chronic inflammation in long Covid patients may damage small nerve fibers. Peter Novak et al., Annals of Neurology
These findings demonstrate that people with long Covid are suffering systemic physical problems, rather than just being anxious or out of shape, said Dr. David M. Systrom, an exercise physiologist at Brigham and Women’s Hospital who helped conduct the bike study.
“You can’t make up small fiber neuropathy by skin biopsy. That isn’t in somebody’s head,” Dr. Systrom said. “You can’t make up poor oxygen extraction to this degree. All of these are objective measures of disease.”
South African researchers found another circulation problem: Microscopic blood clots. Tiny clots that form during an initial Covid infection will typically break down naturally, but might persist in long Covid patients. These clots could block the tiny capillaries that carry oxygen to tissues throughout the body.
Figure: Platelets in the blood can become hyperactivated in Covid and long Covid patients, contributing to microclots. Etheresia Pretorius et al., Cardiovascular Diabetology
Inflammatory substances called cytokines, which are often elevated in long Covid patients, may injure the mitochondria that power the body’s cells, making them less able to use oxygen. Walls of blood vessels may also become inflamed, limiting the uptake of oxygen.
Whatever the cause, low oxygen levels may contribute to long Covid’s most common symptom, severe fatigue. Some long Covid patients meet the criteria for ME/CFS (also known as chronic fatigue syndrome), which often starts after a viral infection. Researchers have found that ME/CFS patients also suffer from a lack of oxygen triggered by circulatory problems. That puts enormous strain on the body’s metabolism and makes simple activities feel like strenuous exercise.
The Brain
“I approach a red light, my brain knows that it’s red, but it’s not reacting to the rest of my body to put my foot on the brake. Do you understand how terrifying that is?”— Samantha Lewis, 34
Even people with mild cases of Covid can experience sustained cognitive impairments, including reduced attention, memory and word-finding. Possible long-term neurological problems from Covid constitute “a major public health crisis,” according to Dr. Avindra Nath, the clinical director of the National Institute of Neurological Disorders and Stroke.
Researchers found a wide range of dysfunction in the brains of long Covid patients. Although it is unclear how often the virus directly penetrates the brain, even mild infections appear to cause significant brain inflammation, according to the researchers, who included Dr. Nath, Dr. Iwasaki and Dr. Michelle Monje, a neurologist at Stanford.
Infections may trigger the over-activation of immune cells called microglia in a way that appears similar to the process that can contribute to cognitive problems in aging and some neurodegenerative diseases.
Figure: Microglia are activated in the brain of a Covid patient, contributing to brain inflammation. Anthony Fernández-Castañeda et al., preprint via bioRxiv. Photos: Myoung-Hwa Lee
Another research group found that long Covid may significantly reduce the amount of blood that reaches the brain, a finding that has was also seen in patients with a related chronic condition, ME/CFS, before the pandemic.
The Lungs
“I couldn’t breathe. It literally felt like someone was sitting on my chest.”— Angelica Baez, 23
Shortness of breath is a frequent symptom of long Covid. But common lung tests — including chest X-rays, CT scans and functional tests — often come back normal.
Using specialized M.R.I. scans, a team of British researchers found preliminary evidence of lung damage in a small group of long Covid patients who had never been hospitalized. Detailed scans of their lung function indicated that most of the patients took up oxygen less efficiently than healthy people did, even if the structure of their lungs appeared to be normal.
The researchers cautioned that a larger group of patients will be needed to confirm the findings. If the results hold up, possible explanations for the observed shortness of breath include microclots in lung tissues or a thickening of the blood-air barrier that regulates the uptake of oxygen in the lungs.
Living With Long Covid
“It’s really not something you can push through.”— Dr. Abigail Bosk
Many hospitals now offer post-Covid clinics or recovery programs, which bring together doctors with experience treating long Covid patients. Given the number of patients, some doctors and programs have long waits for appointments. It can help to plan ahead and try multiple options.
— Americans with long Covid may qualify for disability benefits, although without conclusive medical results, many people face roadblocks.
— Three leading researchers into long Covid often share information about the latest findings on Twitter: Dr. Amy Proal, a microbiologist at PolyBio Research Institute; Dr. David Putrino, the director of rehabilitation innovation for the Mount Sinai Health System; and Dr. Iwasaki, the Yale immunologist.
—Health Rising covers the latest research into long Covid, ME/CFS and other chronic illnesses in detail.
— Gez Medinger, a video producer, interviews some prominent researchers into long Covid on YouTube.
— A video interview with Dr. Svetlana Blitshteyn, a neurologist and the director of the Dysautonomia Clinic, offers advice for treatment and an overview of current research into autonomic disorders.
— A detailed guide to understanding, treating and living with orthostatic intolerance is available from the Johns Hopkins Children’s Center.
Source: by Josh Keller(The New York Times). Illustration by Violet Frances for Bryan Christie Design. Produced by Jonathan Corum. Additional reporting by Pam Belluck and Amanda Morris.
Thinking about how a year ago I was interviewed by a very popular radio show about my long COVID symptoms (I was over a year into experiencing them). They ended up not using my story because “it was too sad” and “I didn’t recover like other people”. They told me to contact them when I had recovered to potentially share my story in the future. I wrote back and told them that most people with long COVID will never recover, and that they weren’t accurately reporting on how COVID affects people. They never replied.
A year later and my symptoms still haven’t improved at all. Anyways, here’s your reminder that the COVID reporting you’re reading (at least in the U.S.) is probably not accurate and is not actually reflecting the suffering of real people.
“We’ll be willing to talk about your chronic illness/disability once you’re over it” is hands down the most abled thing I’ve heard in my life.