#medical discrimination

Update on the situation with my access to the steroid inhaler I need to live…
After a lot of unbelievable screw ups, transmasc discrimination, melodramatic cisgender fragility, manipulative corporate head games, and stonewalling & gaslighting to cover their asses, I finally got the telehealth provider app people to prescribe a 3 month supply of my steroid asthma inhaler… after having to beg and plead the manufacturer on my own to bend the rules to allow me to get renewed into their subsidized prescription program, because the telehealth provider refused to fax in my prescription and the renewal forms to them. The meds are super expensive, and I can’t afford them any other way.
It was a battle after I qualified too, because the telehealth people at first refused to write my prescription, saying they already did, then they sent an Albuterol rescue inhaler script instead of the right prescription to the steroid inhaler manufacturer (who doesn’t even make Albuterol), and when I complained, they said that I was never on the steroid inhaler at all, and lying about it (though there’s a year of records of it with the manufacturer). After much verbal abuse and head games to try to drive me off, I got them to straighten it out. The manufacturer had to rush expedite my prescription to get it to me in time. (The telehealth app people also pulled other related gaslighting and discrimination crap that’s too traumatic to discuss further here)
I’m now stuck searching for a new telehealth provider app. I’d be a fool to risk my life and emotional trauma to go through that crap again… and the reason why I’m using telehealth app services at all is because of violent anti transmasc discrimination locally. I still don’t have access to emergency or local health care because I’m Transmasc in a Deep South state.
…and I wouldn’t even need any of this shit if my bigoted landlord would enforce the posted anti smoke (and p0t) laws in the building where I live. I’d still be running marathons, not bed bound, trying to find a lawyer willing to represent a Transmasc person’s civil rights.
Fucking tired of this shit.
Going through a difficult time right now; prayers, wishes, and good energy sent would be greatly appreciated. Please, people.
In short, I’m having a lot of difficulty getting access to the prescription manufacturers subsidy for the steroid inhaler that’s been keeping me alive for the past year. If I go off it, I will die of pneumonia without access to emergency health care, due to the violent anti Transmasc discrimination where I live.
So basically, I’m waiting to find out if I’m going to be allowed to live, or die, because I’m Transmasc and seen as a not valid life form and an open season civil rights target free from repercussions.
Please… “like” mark in support and send good energy and prayers… the situation is dire.
nah, i’m annoyed enough to make this post.
i am an advocate for finding the right doctor, but seeing a bunch of doctors say “but there are good ones! you just have to find them!” is proof that they are so far removed from the reality of what people (especially marginalized people) experience when going to physicians, psychologists, psychiatrists, etc.
people die because of how doctors treat and dismiss them. poc are constantly treated like they’re lying. fat people do not get listened to because every symptom must be due to weight. addicts are regularly treated less than human or like their health doesn’t matter. women get told they’re exaggerating or are weak. mentally ill people get pills thrown at them after a 15 minute psychiatry session.
i’m not saying people should not try to find a good doctor or that good doctors aren’t out there- my current psychiatrist is fantastic. but a bunch of medical professionals acknowledging how shitty the system is in passing and telling people to just ‘keep trying’ shows how little they understand that patients are too exhausted, too traumatized, and too poor to go from doctor to doctor, hoping one actually takes them seriously.
“If I only had a common illness like diabetes I’d be able to access competent medical care without having to go doctor shopping.”
No, you wouldn’t.
The more time I spend talking shop with other diabetics the more I see doctors routinely screwing up our care and treatment. Everything from bullying us into weight loss to the point of developing eating disorders to withholding needed medication because they’re worried we’ll get fat if our bodies are able to process carbs into energy. People with symptomatic, urgently high blood sugars being given 500mg off metformin and sent home from the ER before they’re even stabilized.
It ain’t about disease rarity it’s about fatphobia, racism, classism, and sexism.
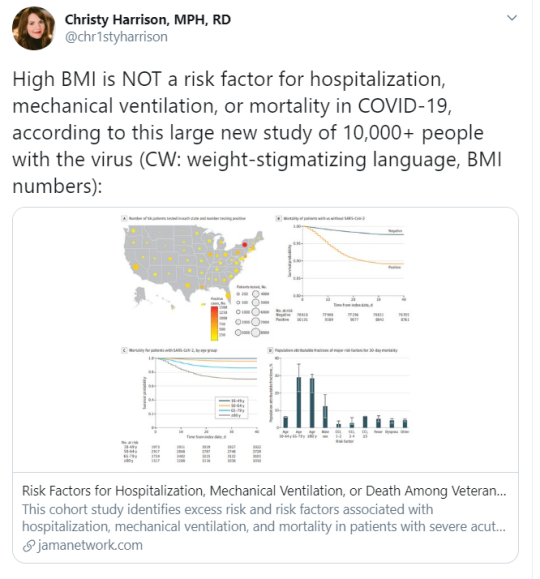
A twitter thread from Christy Harrison, MPH, RD:
High BMI is NOT a risk factor for hospitalization, mechanical ventilation, or mortality in COVID-19, according to this large new study of 10,000+ people with the virus (CW: weight-stigmatizing language, BMI numbers)
I hope we’ll see major media reporting on this study, as it’s one of few studies on this topic to fully adjust for confounding variables, and definitely one of the largest studies that I’ve seen to date on this topic.
Interestingly, it found that although Black patients were more likely to be hospitalized and to receive mechanical ventilation than white patients, they WEREN’T more likely to die.
This may have something to do with equalized healthcare access (this study was conducted in the VA healthcare system) or less-discriminatory care in that system (where the percentage of Black patients is much higher than many other healthcare systems).
Also, Hispanic ethnicity was not associated with increased risk of adverse outcomes in this study, which again may reflect the better access to quality care that patients of color receive in the VA system.
That access and quality may also be why larger-bodied patients fared just as well—and in some cases better—than smaller-bodied patients in this study (see Table 1).
In short, this study supports what I’ve been saying since March: we need to stop jumping to the conclusion that high BMI independently raises COVID-19 risks; when we have good studies that control for confounding variables, those supposed risks disappear. It’s not the weight.
{kind=link}
Another notable point: As is often the case when you account for appropriate confounds like access to medical care and the negative health effects of poverty, underweight people actually have the highest risk of health complications from COVID compared to other weight groups.
still reeling over the fact that epipens aren’t available in doses for larger people and the fact I found that out by nearly dying lmao
this is what we mean when we say fatphobia literally kills people btw





Comic about trans men in the health care system I made for magazine Ottar last autumn! Please note that it presents a Swedish perspective unless stated otherwise, as it is mostly based on Swedish studies. I would however argue that it has implications on the state of healthcare for trans people in other places as well. Thank you so much Hedvig for translating this!
Post link