#multiple sclerosis



day 1/5 experience of 1,000mg methylprednisolone infusion for an aggressive ms flare as of yet untreated. i didn’t sleep more than a half hour last night fearing the treatment wouldn’t work i didn’t fear treatment itself. they say they can’t promise the infusions will help everyone. but it can hit you right away and bring you relief that grows throughout the round. today i walked in public without assistance for the first time in nine months. from my car to a tea house just a tshirt and scrub pants and a chai and sense of euphoria yk me! did not fatigue to tears..didn’t lose my balance.. i felt so much stronger. my mouth tasted so much like metal lol. again tomorrow! each day my nervous system heals and i regain ability. thank hashem for life my amulets were in my pocket the whole time. too giddy to sap cry. might be partly the roids.
summer has already begun here in the us south, and one of the oldest recognized cardinal signs of multiple sclerosis and related conditions is uhthoff’s sign, a sensitivity to heat that triggers symptoms like weakness, pain, coordination and vision problems. symptoms usually dissipate when the body temperature is lowered.
but yk we need to get out too, to walk to work, to get exercise and pt, to enjoy more than a tepid bath and wrath of nerve dysfunction.
the multiple sclerosis association of america has a program giving out free cooling gear for those with ms who meet income requirements.
check it out!!
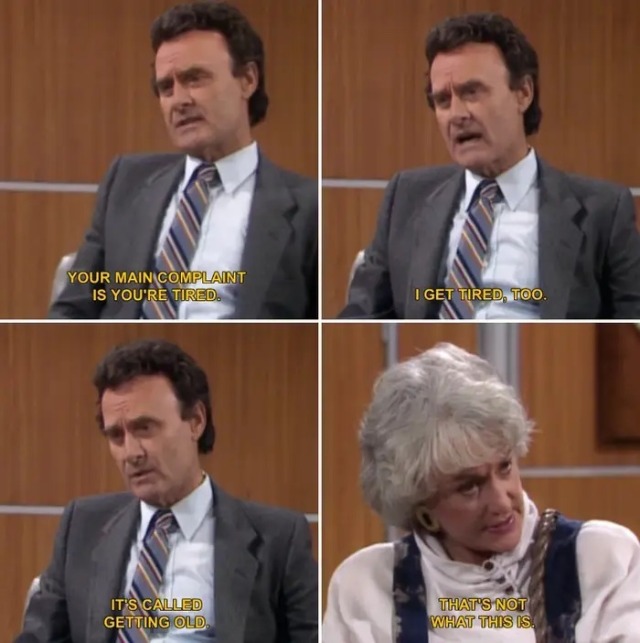
rewatching golden girls “sick and tired 1&2” (1989)

dorothy’s never vulnerable, uncertain, inarticulate or plagued with self-doubt. but in this episode the ensemble’s pillar of strength and wisdom begins to crumble, and no one with the power to help her can (or will) offer answers and relief. she’s sick. doctors tell her she’s fine, that her symptoms are just how everyone feels, when they age or when they’re unhappy. they send her away. dorothy realizes she has to advocate for herself, set her job aside, travel far from home, get second, third, fourth opinions while meanwhile she is too tired to wash her hair in the shower.
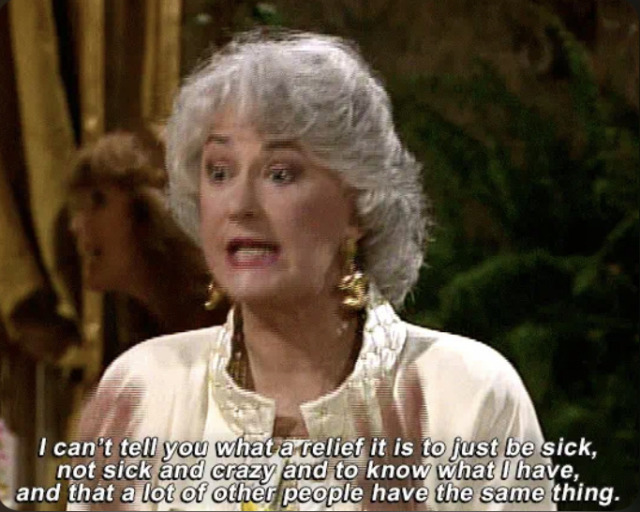
finally a doctor diagnosed her with chronic fatigue syndrome. the news she isn’t ok becomes vindication. validation of the struggles no one else thought were worth their time. dorothy even has the chance to confront one of the providers who failed her and says her piece.
that last bit is a great piece of revenge fantasy for the chronically ill. i revisited this episode after my own bout with diagnostic limbo, and over 30 years later, the frustrations live on. months of “i don’t know what’s wrong” or “nothing is wrong” or “you’re downplaying the role of stress in this” or “you need vitamins” or “you need to see a psychiatrist” or “conversion occurs when…” until a full cns mri and lumbar puncture showed i had inflammation in my spine and lesions all over my brain.
i don’t have chronic fatigue syndrome (though some floated the possibility), i have multiple sclerosis. which, for better or for worse, causes damage to the brain we can see. never was i so relieved to learn i had permanent brain damage and an incurable disease. cuz i knew i could get relief and stop feeling crazy.
almost every woman* i know with ms tells the same story: doctors were dismissive and told them they were on some spectrum of tired to stressed to hypochondriac. they got sent to a therapist before getting an mri. if depression were the primary presentation of ms, id understand, but there’s infinitely more. many of us go blind and/or lose the ability to walk. and they will still say to see a psych before even examining us.
early detection of progressive diseases like this matters because you cannot reverse brain and spinal damage from ms. you can only slow progression, calm flares, and treat symptoms. early detection is so important, so why don’t doctors take their patients more seriously?

little detail of this episode—the input from friends as to how dorothy should look for her doctors appointments eg how much makeup, to make her look the part of a sick patient, while the top neurologist writes her off and suggests she dyes her hair and revitalizes herself inside out. how many of us contemplate how “together” we will look in the hospital! will makeup make them like us more? does this outfit say im trustworthy? should i brush my hair when doing so makes my arm too tired i have to rest a couple hours? games u know are absurd as you play them

take away—feeling crazy and helpless is normal but it doesn’t mean you are crazy and helpless. if something is off, please don’t delay getting help, cuz the rest the world will definitely find ways to keep you from getting the treatment you need. your pain is real, and you deserve answers.
*around 75% of people with ms and cfs/me are women
 of MS is still not kn")
 of MS is still not kn")
What causes multiple sclerosis?
While the cause (etiology) of MS is still not known, scientists believe that a combination of several factors may be involved. Studies are ongoing in the areas of immunology (the science of the body’s immune system), epidemiology (that looks at patterns of disease in the population), and genetics in an effort to answer this important question. Understanding what causes MS will be an important step toward finding more effective ways to treat it and—ultimately—cure it, or even prevent it from occurring in the first place.
The major scientific theories about the causes of MS include the following:
Immunologic
It is now generally accepted that MS involves an immune-mediated process—an abnormal response of the body’s immune system that is directed against the myelin (the fatty sheath that surrounds and insulates the nerve fibers) in the central nervous system (CNS—the brain, spinal cord and optic nerves). The exact antigen, or target that the immune cells are sensitized to attack, remains unknown — which is why MS is considered by most experts to be immune-mediated rather than autoimmune. In recent years, however, researchers have been able to identify which immune cells are mounting the attack, some of the factors that cause them to attack, and some of the sites, or receptors, on the attacking cells that appear to be attracted to the myelin to begin the destructive process. Ongoing efforts to learn more about the immune-mediated process in MS—what sets it in motion, how it works, and how to slow or stop it—are bringing us closer to understanding the cause of MS.
Environmental
MS is known tooccur more frequently in areas that are farther from the equator. Epidemiologists—scientists who study disease patterns—are looking at many factors, including variations in geography, demographics (age, gender, and ethnic background), genetics, infectious causes, and migration patterns, in an effort to understand why. Studies of migration patterns have shown that people born in an area of the world with a high risk of MS who then move to an area with a lower risk before the age of 15, acquire the risk of their new area. Such data suggest that exposure to some environmental agent that occurs before puberty may predispose a person to develop MS later on.
Some scientists think the reason may have something to do with vitamin D (.pdf), which the human body produces naturally when the skin is exposed to sunlight. People who live closer to the equator are exposed to greater amounts of sunlight year-round. As a result, they tend to have higher levels of naturally-produced vitamin D, which is thought to have a beneficial impact on immune function and may help protect against autoimmune diseases like MS. The possible relationship between MS and sunlight exposure is currently being looked at in a Society-funded epidemiological study in Australia.
Other scientists study MS clusters—which are defined as higher-than-expected numbers of cases of MS that have occurred over a specific time period and/or in a certain area. These clusters are of interest because they may provide clues to environmental (such as environmental and industrial toxins, diet, or trace metal exposures) factors that might cause or trigger the disease. So far, cluster studies have not produced clear evidence for the existence of any triggering factor or factors in MS.
Infectious
Since initial exposure to numerous viruses, bacteria and other microbes occurs during childhood, and since viruses are well recognized as causes of demyelination and inflammation, it is possible that a virus or other infectious agent is the triggering factor in MS. More than a dozen viruses and bacteria, including measles, canine distemper, human herpes virus-6, Epstein-Barr, and Chlamydia pneumonia have been or are being investigated to determine if they are involved in the development of MS, but none have been definitively proven to trigger MS. Read more on viruses as the cause of MS
Genetic
While MS is not hereditary in a strict sense, having a first-degree relative such as a parent or sibling with MS increases an individual’s risk of developing the disease several-fold above the risk for the general population. Studies have shown that there is a higher prevalence of certain genes in populations with higher rates of MS. Common genetic factors have also been found in some families where there is more than one person with MS. Some researchers theorize that MS develops because a person is born with a genetic predisposition to react to some environmental agent that, upon exposure, triggers an autoimmune response. Sophisticated new techniques for identifying genes may help answer questions about the role of genes in the development of MS.
photo one source
photo two source
Post link
I was recently yelled at by a man driving by as I was walking into a Starbucks after parking in a handicap spot. “Liar! Liar!” My first thought was “you weenie come back and say that to my face!” Then the shame set in. For awhile I felt guilty of…something. I know I’m sick but I know I don’t look sick, so maybe I don’t deserve my placard? It’s confusing and I understand. But then I reminded myself that 96% of chronic illnesses are invisible. Just because I look fine doesn’t mean my illness goes away or isn’t serious enough to be disabling. It’s not me that’s somehow confusing or misleading, it’s society and our expectations and stereotypes. Sick doesn’t have a look and neither does disabled. This idea that to be valid your illness or disability must be visible is ludicrous when you learn how many people are suffering from something unseen. Society needs a major reform in many ways, but especially with respect to its treatment and expectations of chronically ill and disabled people. What we really need is to just stop being so dang judgmental in general! Was it ever any of his business where I parked or if I “deserved” my license plate? No sir! All that I ask of people at this point isn’t even kindness, just neutrality or even indifference! Let me be! Can I just get my chai in peace?!







Multiple Sclerosis Is Likely Caused by a Virus, Finds Study of 10 Million Military Personnel
Aaaaaah, this is such important and good news.
As someone with complex health needs, it really is heartening to finally see so much progress being made with research and the results finally confirming what many of us suspected: that our complex ailments are the result of viral infection.
Still an absolute mother fucker for those affected, but still, progress!!
Please open and read the article, because the headline doesn’t do the results justice at all:
Becoming EBV-positive resulted in a 32-fold increased risk of later developing MS as opposed to remaining EBV-negative. The next-strongest known risk factor for MS is having a set of genes that encode for proteins found of the surface of certain immune cells. People with a particular set of these immune cells, who have a homozygous genotype for the HLA-DR15 allele, have a threefold increased risk of MS.
That is. Do you know how ludicrously strong a result that is. And they did some clever analysis to prove that it was EBV (mononucleosis/glandular fever) rather than any confounders:
Ascherio’s team examined antibodies against cytomegalovirus, another saliva-borne virus that has also infected most of the world’s population, to serve as a negative control. Individuals who were CMV-negative at their first sample showed no increased risk of MS if they later became CMV-positive.
MS is thought to have a long prodromal phase, meaning the disease could affect the immune system years before symptom onset and diagnosis. Could the EBV-MS relationship be reversed? Perhaps people who have MS but don’t yet show symptoms are more likely to develop an infection such as EBV. To rule this out, Ascherio’s team looked at 30 MS patients, and 30 healthy controls. They used a search tool called VirScan that enables the detection of any antibody raised against any protein in any of the ~200 viruses known to infect humans. The only virus to show significantly increased presence in MS cases was EBV.
Like, I have a degree in statistics, and I am comfortable with saying that this paper has shown that EBV causes MS. And in excellent concurrent news, Moderna has just started phase 1 trials of an mRNA vaccine against EBV! The future is now!
There’s actually been a lot of recent advances showing that ailments we had a hard time understanding or treating before are actually due to variant immune responses to one of the nine human herpes type viruses [The family that included EBV HSV and Chicken pox] and that these conditions are also far more common than previously thought.
As a side note to do with Corona, and these viruses [together], which is just personal observation from my own life, and the people around me, and should be taken as such:
I -personally- have noticed a trend of people who have been infected with corona suddenly developing worsening symptoms or life-threatening health episodes caused by these other viruses, and suspect that Coronavirus does something that affects some people’s immune response to these existing viruses, because the number of people around me who suddenlydeveloped shingles, or suddenly developed viral meningitis [diagnosed as being HSV despite that they’ve had that since high school and are grandparents now], or suddenly had symptoms that would align with one of these viruses causing nerve damage or even affecting their vision -all only after having been exposed to corona virus, or all after the pandemic started regardless of symptoms of covid- is just WAY too damn many to be a coincidence, for conditions and complications that are supposedly so rare that my doctors won’t explore them properly.
It seems to be doing something to affect the normal/healthy ability for people’s immune systems to suppress these viruses -which stay in the body- the way they regularly would, and the doctors around me seem to be really resistant to admitting it is a problem even once they are forced to diagnose and threat the abnormal symptoms of these herpes family viruses spreading places they shouldn’t. I’d put money on them trying to avoid a huge panic and a huge uptick in demand for antivirals right now, even if it means under-treating patients who might go blind or might have recurrent viral meningitis.
Fibromyalgia was already thought to be a complication of the long term, and even ongoing, nerve damage caused by the chicken pox virus. It was alreadysuspected that a lot of cases of recurrent meningitis were actually viral and should not be being treated with antibiotics at all. Progress on this has been slow but the evidence is there.
And while it’s speculation on my part, I’m going to betthat the number of people who develop complications from EBV or HSV or Chicken pox is about to SKYROCKET, and the percentage of people diagnosed with fibromyalgia, MS, chronic fatigue and other chronic viral inflammation is about to as well. To the point where the world will be forced to treat these viruses as the public health crisis they have beenforsome of us all along. The problem is easy to ignore and downplay when it’s just a few people -and mostly women- becoming so disabled they can’t live normally, but what percentage of the population suffering from these things does it take for there to be systemic change in how it is diagnosed and handled?
And I wonder how much the ‘Trumpets’ who are insistent on partying and not taking this virus seriously would suddenly change their tune if they realized it could mean having huge visible cold sores or herpes outbreaks suddenly be a monthlyexperience for them for the rest of their lives, or could mean one of those viruses might suddenly spread to their eyes, lungs or brain when they were previously healthy and previously had a proper immune response. All in a pandemic with doctors who already refused to take those possibilities seriously enough to treat them in time to prevent disability and death and who are currently run down and exhausted of all energy or resources.
oh, yeah, my dad got COVID and it unvaccinated him. he got the shingles vaccine and nope! covid undid it and he was having shingles symptoms right on the tail of his covid symptoms. bad ones, too- trigeminal neuralgia in the face. I think there’s some other folks who have similar stories of people getting covid and losing immunity to viruses or post-viral symptoms.
(also- do most people not get monthly cold sores? is that abnormal?)
Multiple Sclerosis Is Likely Caused by a Virus, Finds Study of 10 Million Military Personnel
Aaaaaah, this is such important and good news.
As someone with complex health needs, it really is heartening to finally see so much progress being made with research and the results finally confirming what many of us suspected: that our complex ailments are the result of viral infection.
Still an absolute mother fucker for those affected, but still, progress!!
Please open and read the article, because the headline doesn’t do the results justice at all:
Becoming EBV-positive resulted in a 32-fold increased risk of later developing MS as opposed to remaining EBV-negative. The next-strongest known risk factor for MS is having a set of genes that encode for proteins found of the surface of certain immune cells. People with a particular set of these immune cells, who have a homozygous genotype for the HLA-DR15 allele, have a threefold increased risk of MS.
That is. Do you know how ludicrously strong a result that is. And they did some clever analysis to prove that it was EBV (mononucleosis/glandular fever) rather than any confounders:
Ascherio’s team examined antibodies against cytomegalovirus, another saliva-borne virus that has also infected most of the world’s population, to serve as a negative control. Individuals who were CMV-negative at their first sample showed no increased risk of MS if they later became CMV-positive.
MS is thought to have a long prodromal phase, meaning the disease could affect the immune system years before symptom onset and diagnosis. Could the EBV-MS relationship be reversed? Perhaps people who have MS but don’t yet show symptoms are more likely to develop an infection such as EBV. To rule this out, Ascherio’s team looked at 30 MS patients, and 30 healthy controls. They used a search tool called VirScan that enables the detection of any antibody raised against any protein in any of the ~200 viruses known to infect humans. The only virus to show significantly increased presence in MS cases was EBV.
Like, I have a degree in statistics, and I am comfortable with saying that this paper has shown that EBV causes MS. And in excellent concurrent news, Moderna has just started phase 1 trials of an mRNA vaccine against EBV! The future is now!
Yay, as someone currently experiencing an Epstein Barr flair I’m so happy. Please enjoy my dripping sarcasm and mild horror of yet another thing Epstein Barr can do to me.
Can I get one last round of motivation?
Today is my very last day I am allowed to get my things from the house to move them to storage or my new apartment. I also have to clean.
This has been hell on earth and I am SO exhausted and sore. This MS is kicking my actual ass.
I’ve still got a bit to do and have all but run out of space in my tiny apartment soo……. Please wish me luck? ❤️
I’m so over all this moving mumbo-jumbo… especially while also working during the busy holidays doing 23 haircuts a day on average with my MS.
I’m so tired and sore I just wanna jump off a cliff …
I need moving motivation please help!!!!
I have to get packing and get stuff moved but my neurological disorder and chronic pain and fatigue has made me sore and tired even right after waking up (as always).
I’m basically doing all this alone and I need so much help I need a buddy to tell me I got this and push me to get going and stay motivated.
Please help!

first dose of gilenya under observation was chill. i don’t miss daily injections but headaches are a sneaky bitch of a side effect that never sound bad on paper until you’re living it
Post link

Trapped in a life that wasn’t meant to be mine.
Imprisoned by the need to be loved.
A body lacking the drive to pursue…anything.
My ‘poem’, not my art (http://art.tavsiyebilgi.com/art-sketches-tumblr-buy-minimal-line-art-woman-with-hands-on-face-art-print-by-nadja1-worldwide-shi-kunstskizzen-skizzenbuch/)
Post link
-Alemtuzumab year 2
This year has definitely been easier than last year was! My younger sister came to stay for a week and helped me with everything which did make life that little bit easier. She did the same last year too; what a star! Thanks Flea!! Don’t get me wrong, I’m super tired and could really do with doing very little for a while (or my sister back? haha) but I’ve been back at work for a week now and it didn’t kill me!
I have had a lot of tingling in my limbs (a.k.a. altered sensation), not something I’m that used to, and headaches on and off…but apart from that & a couple of little blips, it’s been ok.
All I have to do now is avoid catching anything and I’ll be happy!
– Days 1, 2 & 3
Here’s a quick update to changes to the treatment plan for this year:
1) The ‘anti-listeria’ diet we are asked to follow has been extended to a month before the treatment starts. We had of course been told this prior to this meeting, but she explained that it was because there had been a death caused by listeria in a patient receiving Alemtuzumab. (Thank goodness I’d followed the instructions, hey!)
2) We would be taking a second tablet (in addition to the acyclovir) home with us this year; it’s an antibiotic called Co-Trimoxazole (2x480mg a day for 30 days, each containing: 80mg Trimethoprim & 400mg Sulfamethoxazole), which has been shown to decrease the risk of getting ill whilst our immune systems are very low.
So, for the second round of Alemtuzumab I had 3 days of treatment. I’m not entirely certain why it’s shorter than the first year, but I do know that this is the standard protocol. This year wasn’t very different from last year except, I suppose, that it was a little easier. I’m not sure if that was because I knew what to expect, or that fewer days meant that my body felt less bombarded (or maybe a bit of both?), but either way, I was glad for it!

(This is Morriston the sloth (named after the hospital that my neuro team are based in) sitting in the chair that was my home for the three days of my treatment this year.)
Day one
We started today with some introductions: Mark & I had a new buddy this year called Jenny (also in her 2nd year) and we all met the new neurologist that has been added to our neuro team; both were great. We then each had a little consultation with said neuro who just went through a few things and did a quick series of tests. All we had to do then was wait for the results of our urine tests, take an antiviral & antihistamine, to be cannulated and we were good to go.
There was around an hour of steroids and then 4ish hours of the Alemtuzumab, followed by 2 hours of observation and a blood test. We had half-hourly obs all day and we mainly looked after by 2 nurses. The unit we were in was being shared with the renal department so there was a steady stream of their patients coming in and out for various treatments all day.
I spent this day in quite a lot of discomfort but I knew it was to be expected. The nurses gave me some paracetamol and said that it was good because it meant it was working. At the time all I wanted to do was cry, but looking back on it that was the worst part of the treatment this year and it really wasn’t that bad.
Mum & I stayed in a hotel again as it was much easier and safer to be near the hospital. I was pretty tired after the first day but when trying to sleep I became VERY restless.
(Cannula number 1)
Day two
I had kept the cannula in from the day before so today started a lot faster than the first. All I had to do was wait for my urine test to show all clear and for the blood results from day one to confirm that the treatment had done what it was meant to do. Both were fine, so, after taking an antiviral and antihistamine again, off we went. I had a headache this day and was quite sleepy, but that was pretty much it.
(Half of the obs sheet from day 2)
Day three
I’d kept the cannula in again for this day but about 30 minutes into the steroids it had to be taken out and replaced on the other side. It was a little painful and the infusion seemed to be going quite slowly so it was decided that it was best to change it. Turned out that was a good idea as when it came out the tube was so bent they didn’t even know how it had been going through in the first place (haha). Apart from that the same morning routine from the day before was followed. I was a little flushed this day and had a bit of a temperature but they both went down by the end of the day. I was a lot more tired so spent a lot of the day in and out of sleeping. I did get a small rash, but NOTHING compared to the one I got last year!
So, that was Round 2…hopefully my last! I have a check-up appointment with one of my neurologists in a month and will have an MRI in June(ish) and then we’ll go from there. Keep your fingers crossed for me!
I just wanted to add a quick thank you to my Mum, sisters and friends that looked after me and messaged me throughout these 3 days! Oh, and the awesome neuro team at Morriston (thank goodness for the NHS!!)!
I haven’t had to update this in a while, which has been good, in this case no news really has been good(ish) news.
So what’s happened since last April? To sum up:
> I caught so many bugs it was unbelievable, but none of them caused any hospital visits and as my immune system regained its strength I did stop catching everything.
> I have Trigeminal Neuralgia & take Carbamazapine to stop it from causing me pain, which coincidentally has also seemed to help my back problems.
> I still have to use crutches every so often, but much less than I was starting to use them.
> I’ve had 3 mysterious skin allergic reactions (as shown in previous post), around 10 issues with my eye - itching/pain - that was stopped by piriton - & now have very dry skin/eczema on my eyelids (Aveeno cream clears it up within 24 each time). The GP I saw has suggested that this is all an allergic reaction to the TN meds, but the TN is definitely still worse than all of that. I’m yet to see if my neuro agrees…
> I had a 2 week spell of headaches behind the eyes couple with some mild vertigo recently, but optician couldn’t find an issue, neither could the GP. Again, yet to really bring it up with anyone on the MS team.
> Fatigue, stiffness and memory issues are unfortunately still ever present, but I think they might be something that stick with me for ever to be honest.
> There have (of course) been other issues here & there, but right now none spring to mind…
I’ve got my date for round 2 of my treatment: 24-26/04/17. To be honest, I’ve had it for a while but have been forgetting to update this blog…
I have so many emotions running around inside of me I’m not sure where to start, all I can say for certain is that I’ll be glad when it’s done with…until then, wish me luck!
Ok, so I’ve now had an allergic reaction twice in the same month. To what you may ask? I really don’t know. Having thought about the 2 days, not much was similar, the reactions happened at different times of the day, 1 took at least an hour to properly kick off, the other maybe 10 minuets…
I’m not sure if these have anything to do with Lemtrada or indeed MS full stop, but they are random and up until now I’ve not had a reaction to anything (except when having the iv infusion) since being a baby.
Just in case you’re wondering what the reaction looked like:

This was all over both arms, my face, upper back & chest. This was the least mentally scarring picture I could find, but mine was quite a lot redder and the bumps were a bit bigger and whiter.
Hopefully the reaction will either not come back, or I’ll find out what’s causing it. Luckily, both times, antihistamine eventually made it subside.
I went to the MS Life event in London this year. I was only able to go for one of the two days, but it was definitely worth it. There were so many different companies and organisations there and I learnt a lot about the help and information that was out there. I won’t go into everything that was there, but its worth looking up & attending!

One of the most interesting resources I found there was the MS Register (https://www.ukmsregister.org/Portal/Home). My neurologist had told me about it before, but whilst at the event I actually got round to joining. It’s a resource that will hopefully help with medical professionals understanding both MS itself and how it truly affects & effects the patient.
First things first, my 6 month lymphocyte count is 0.9 - nearly within ‘normal’ range according to my neurologist and is definitely a good thing.
My appointment gave me the opportunity to bring up a few things I’d been worried about/experiencing. Nothing too bad, just a few things that may need more attention next year.
I was also able to catch up briefly with Mark (we had Lemtrada at the same time) which was good. He’s doing well too. We both have to have the Flu jab this year - something I’m definitely not looking forward to.
I’m now taking 50 mg of Carbamazapine twice daily to help with the trigeminal neuralgia - something which my neuro said was a MS thing, but when someone with MS has it, it’s a bit different (it’s caused by the demyelination). It’s being caused by one of my original lesions, so nothing to worrying about on that end (in other words: it’s not new).
This is an amazing talk from an inspirational woman that has had Lemtrada.

It turns out that the face pain I’ve been having is something called trigeminal neuralgia. It had become more frequent so I finally went to the doctors. It isn’t necessarily to do with MS or the treatment, but it is VERY common in MSers. At the moment I’m not taking anything for it but we’ll see a couple of weeks from now.
I just thought I’d write a quick update, I suppose this one is more for me (so I have a chance of remembering)…
On 3 or 4 separate occasions (including my birthday) I had a HORRIBLE pain down the right side of my face. The longest ‘attack’ lasted on/off for about 1.5 hours, but it would appear that rotating the skin near my temples helped disperse it, but not always completely. Like this:

I’ve also had a bit more trouble with my legs and back. Stiffness & pain have been an issue for over a year now, but it was ‘getting better’. I’m not sure if it’s worse than it was, or I that I had gotten so use to not having the problem that having them back just feels worse. I am waking up with some stiffness now which is definitely new (it used to ‘disappear’ overnight).
My memory seems to have gone downhill a bit too, but that was rubbish to start with, MS aside… The fatigue is also a big problem, but I think that’s probably pretty normal to be fair.
My consultant did say that things might have to go down hill a little before getting better. I’m always being reminded that Lemtrada isn’t a quick fix and believe me, I know it!
[19 weeks, 2 days post R1]
I had my first successful Facetime urine dipstick test today! This might seem like a strange thing to be excited about, but my phone wouldn’t work last month so getting the test done ended with me going to my local minor injuries department just to be able to get it done - what a palaver!
Just in case you’re wondering….

I was given a bottle of dipsticks and a print out of the chart to compare my results with. My MS specialist nurse then contacts me via video chat so she can see the results herself too. I do the test and compare the results, telling my nurse (Bernie) what I think they are.
I’m pretty used to doing this type of thing as I have a similar test for the water in my fish tank, so this works quite well. Also, it save at least 2 hours driving/missing work/money so is a great way to do this test!
Thank goodness for modern technology right?
A new poem about identity and facework and the misconception that there is privilege in being visibly disabled. Performed at the Portland Poetry Grand Slam. Filmed by SlamFind.
can someone please do a transcript for this? the auto captions are okay but I think some things are missing and I can’t get them and I want to.
Transcript:
“after Crystal Valentine
I used to be scared to call myself disabled
because I didn’t look the part
but the disability is my performance of it
my performance is always the loudest thing in the room
even when I am silentI show up with a wheelchair and an honest body
and I do not need to say
I am disabled
you already believe itThis is visibility privilege
I bring the wheelchair to a benefits interview,
when it’s more convincing to wear my impairments
than explain a diagnosisThe midnight hospital trips
when the pain has taken everything I have
I bring the black cane, that folds, that says
I am a serious patient, the illness is so much
a part of me I accessorize with itBut the next morning, picking up prescriptions
in the store where I used to work,
I take the hospital cane even though it is heavier
I say I am injured, not ill
all this I call temporaryThis is passing privilege
A stranger asks if I have gotten better when I stand onstage unassisted
in the only 2 hours all week I will leave my bedAnd this is erasure
Just yesterday, it seems
I was whole person
with a job and a life and
now everything is disappearingThe first time my arm was too weak
to lift a full cup from the bedside table and it spilled,
I just sat there, coffe soaking the sheets
tears falling down a face I couldn’t feelA hospital full of doctors, and not one can tell me
when I will die, just that it will be too soon
anything I hold could be dropped in an instantI’m not startled anymore by the sound
of porcelain shattered
cleaning up another murdered dish
I remark to the empty apartment
how strange it is to watch these hands that once
built houses now break everything they touchLast week a new doctor said
I read your chart, you’re a climber?
so am I
I said, I used to be
and now this silence is all that’s shared between usAnd this is cripple privilege
the only power I have left
how easily I can make you pity me”[video description: Erin Schick (pale, thin, short/buzzed auburn or brown hair, no glasses) is standing in front of a microphone on a dark stage. they’re wearing a dark green or gray shirt. the video is filmed from the side.]
I’m nowhere near this bad (thankfully) but I can definitely identify with a lot of what she says!
