#medical school

![cranquis:thuc:The Dedicated Doctor [infographic]No doubt about it, becoming a physician is har](https://64.media.tumblr.com/1c8797d5094eea77bd148fd10fe5cf38/tumblr_mlapd3sjOf1qzjvqlo1_r1_640.png "cranquis:thuc:The Dedicated Doctor [infographic]No doubt about it, becoming a physician is har")
thuc:
The Dedicated Doctor [infographic]
No doubt about it, becoming a physician is hard work and a long road. Healthcare reform is here so…
An inspirational infographic by the Alpha Infographicist thuc.
One not-so-inspiring comment, though: yes, more doctors are needed, yes, more spots are opening up in med schools, more jobs will be available for med school graduates, more patients are going to become insured under Obamacare — BUT since jack-squat is being done about proportionally improving reimbursement for all those doctors (new and old) and alleviating the massive debt which med students have to incur in order to become underpaid doctors, it’s still going to be tough to keep those doctors in business. Because it IS a business.
/rant
Post link

Everybody is talking about it. It’s shaping up to be one of the worst flu seasons in years. And, with all the commotion It never fails, we hear it every year-“Nah man, I don’t mess with the flu shot! The last time I got it, it gave me the flu!” Or, the always classic “Why would I get that shot again? Last year I got it, and still got the flu!”. With that being said, we decided to sit down and put together a short article on why getting the flu shot won’t give you the flu, but also why it can’t guarantee you won’t get it either.
THE BASICS:Without getting too “sciency” on you, lets talk about the flu shot itself. When you get a flu shot, what you’re actually getting is what’s known as a “dead virus”, which means the virus in the shot is, well, dead. “There is simply no way that the flu vaccine can give you the flu,”saysChristine Hay, MD, assistant professor at the University of Rochester Medical Center. “It’s impossible” (we’ll explain why it’s impossible later).
“WHERE MY DOGS AT?”: At this point, you’re probably wondering to yourself, if what’s in the flu-shot is “dead” then what’s the point of getting it, right? Fair question, and here’s a simple way to think of it. Your body has its own defense against “intruders” (i.e. your immune system), you can think of these as guard dogs, running throughout your body, attacking suspicious looking characters who might otherwise do you harm. These guard dogs have been trained to sniff out your run-of-the-mill “home intruders”, so most of the time when an intruder (playing the role of a virus in our scenario) tries to make its way into your body, your dogsare on the prowl and ready to handle your dirty work!
There’s only one problem in this hypothetical scenario. Every year the home intruders get a little more clever, and they switch things up. Maybe they ditch the ski mask, its too obvious. Instead, this year they decided to roll with the hoodie instead, it’s a little less suspicious. Now imagine the intruder makes his way inside your house, and it isn’t until he starts wrecking shop that your guard dogs realize “Aww snap! We have a problem here!” at which point they jump into action and try their best to control the situation. But, they’re a little late to react to the intruder (they didn’t know what to make of their new disguise at first), and he was able to break a few things and got away with some property.
Granted, the dogs eventually sprung into action, but the damage had already been done. They only upside to this scenario is that if the home intruders come around again, dressed similarly to the recent intruders (i.e. wearing hoodies), your dogs will be ready to spring into action.
FLU-SHOT IN TRAINING: What the flu shot does is basically offer up “training” for your guard dogs. The three most common “looks” for home intruders in your neighborhood are identified, rag-doll versions of them are made, and dressed to look exactly like them. The dogs are then introduced to the rag-doll intruders, and trained to attack them on sight! Even if it takes them a little while to be trained (just like it takes the flu shot a few weeks to “kick in”), it’s okay because the rag-dolls pose no threat, they’re not real, just as the dead virus in the flu-shot is not a threat.
The idea is this: Now that the guard dogs know what they’re looking for, if and when the actual intruders show up, there will be little to no delay in attacking, and shutting them down! With no time to wreck shop, the bad guys stand little chance to do any harm to the home or the people inside!
SO, WHY DID I STILL GET THE FLU LAST YEAR?: Now that you (hopefully) have a little better understanding of why we get flu shots, and how they work, lets talk about why some people still get the flu, despite having received their shot. One explanation is simply that (again, continuing with our guard dog and home intruder analogy from above) the home intruder was not dressed like one of the three included in the vaccine. Makers of the the flu-shots do their best to identify the top three strains they think will most likely be infecting people in your area. However, there is no way they can possibly account for allof the flu strains (just like it would be impossible to guess what everypotentialhome intruder would look like). But, life is all about percentages and odds, so the idea is to stack the odds in your favor: If you’re at risk for catching the flu (which we all are), here are the most likely critters to get you, and here is a vaccine against those strains. It’s that simple.
A more obvious explanation can be that you were exposed to the flu virus before you received your shot, or in the two weeks it takes for the shot to start protecting your body. Lastly, some people just love a good conspiracy theory, and at the first sign of a sniffle or a cough, will mistake their symptoms for the flu instead of what it actually is, a simple cold.
Injury-Duty Insight:There you have it. Now you know how the flu shot works, and even why it sometimes doesn’t. Keep in mind that flu seasonin the United States tends to start around November and continues to peak all the way through April, so there’s plenty of reason to still go out and get yours, should you want it. Also keep in mind that children (over 6 months) and elderly (over 65 years old) should be first in line to get their shots, because the babies, well their guard dogs are just puppies (they need all the training they can get!) and the older folks, well their guard dogs don’t react as quickly as they used to, so they need all the head-start they can get!
(Like What Found Here? Have Comments, Questions? Concerns? Visit Out Injury-Duty Facebook Page of Follow Us On Twitter @Health_ID)
Sources:
1. Christine Hay, MD, assistant professor, University of Rochester Medical Center, Rochester, N.Y.
On September 8th 2012, TulanesafetyDevon Walker (21 years-old) was left paralyzed after he fractured his spine in a head-to-head collision with a teammate during a game in Tulsa (video: click here). Since then, we’ve overheard people talking about his injury, whether it be in the hospital or at the grocery store. And, the one big thing that has seemed to connect the conversations: Misinformation. So, we decided take a closer look at spinal cord injuries in football, in hopes that you (both parents and players) might find something here helpful.
SPINAL ANATOMY:Your spinal cord is directly connected to your brain. If you were to remove all that surrounded your brain and spinal cord (all the skin, muscle, bone, etc.) the spinal cord would sort of look like a ponytail dangling from the base of the brain. Now, if you imagine your spinal cord is a cooked spaghetti noodle (which is actually pretty close to its real consistency), imagine putting that noodle through the opening of one of those bendy straws (see diagram below). What you would now have is not some bullet proof protection around the noodle, but you’d definitely have protection around that noodle making it less likely to be cut or torn when it’s being hit. That is essentially what your spinal cord is, a noodle with a thick covering (the nerd-term for the thick covering is the “dura mater”), hanging from the base of your brain.

Thespinal cord itself serves as a “highway for information” that carries information from the “outside world” (for example, pain from touching a hot stove) to the brain and also carries information being sent out from the brain to the rest of the body (for example: the command to extend your arm and reach for something). All of your thoughts that eventually become actions (moving your arms, legs ect.) and even some things you don’t ever have to consciously “think” about (blood pressure, heart rate etc.) are all (at least partly) controlled via commands form different centers in your brain. Those command signals travel down from your brain and to their eventual targets. Being that this cord is such an important structure, you’re body is designed in a way that it tucks your spinal cord behind a lot of protection, mainly your vertebral column (aka your backbone or spine).
The spine itself isn’t just made up of one long bone though, instead it’s made up of vertebrae. Think of the vertebrae as individual building blocks stacked one on top of the other, with padding in-between each block (the pads are called “Intervertebral discs”, in nerd-speak), which are soft gummy-bear-feeling type discs made to adsorb the impact between your vertebrae.

Youractualspinal column is made of bone and is divided in to 3 “sections”:
1. Cervical spine (your neck; you have 7 vertical vertebrae or “blocks”)
2.Thoracic spine (your mid-back; you have 12 vertical vertebrae )
3.Lumbar spine (your lower-back; you have 5 vertical vertebrae )

The vertebrae (the “blocks”) become larger as you go further down your spine, and there are a couple of reasons why this is the case. First, the lower vertebrae have to support more of your body’s weight, so it makes sense that they’d be “beefier” and more heavy-duty compared to the higher vertebrae in your neck, which most often only have to worry about holding up the weight of your head. The second reason the vertebrae in your neck are smaller is because as humans we depend on our eyes and ears to keep us aware of our surroundings, and those eyes and ears are attached to your head (obviously). Each time we turn our heads, a complex network of muscles, tendons and ligaments that are attached to our vertebral column pull on the specific vertebrae we need to move, which in turn helps to turn our head. If those vertebrae were big, they’d require a lot of energy to pull on and we’d be straining ourselves every time we wanted to simply turn our heads.
Now, going back to our bendy-straw and blocks analogy, if you imagine the bendy part of the straw being your neck, you’ll realize that you have a lot of mobility there. But, your neck is a lot thinner than your chest or waist is round, which again, is great for mobility but not so great in terms of protection for your spinal cord. All that freedom to move around makes your neck more susceptible to being pushed or pulled too far, which brings back to Devon Walkers injury.
The Specifics Of Walker’s Injury: Devon Walker suffered a fracture of his cervical spine (a “broken neck”). As of the time this article was written, where exactly along his cervical spine his injury happened has not been made public.
Early Reports:Several news sources were reporting that Devon “stop breathing” after the injury and that he required CPR while on the field. We have not been able to confirm if Devin did in fact stop breathing, or if his breaths only became very shallow (for reason’s we explain later).
Understanding The Injury:As we explained earlier, the spinal cord both caries information from the “outside” to the brain and also sends information from the brain to the rest of the body. Along the spinal cord there are “exits” where “spinal nerves” branch off, think of these as “off-ramps” from the “main highway” (the main highway being your spinal cord). Each spinal nerve, depending on which level it makes its exit, is responsible for carrying signals to things in that general area.
As you now know, the spinal column is divided into three sections (cervical, lumbar and thoracic), and each of these sections have a specific number of “exits” where spinal nerves branch off (see diagram below). In Devon’s case, we know that the injury was to his cervical spine (vertebrae in the neck). As you can see in the diagram, the signals that exit the spinal cord at that level are those that control the head, neck, upper arms, hands and breathing muscles (namely the diaphragm); the diaphragm is a large muscle located “underneath your lungs” that allows you take a deep breath).

Had Devon’s injury only damaged the spinal nerves at that level, he’d most likely have use of his body below the area that was damaged, because the spinal cord itself would have been left undamaged. Unfortunately for Devon, he was unable to move his arms and his legs after the accident, which suggest that the injury was bad enough that all “signals” below the level of his injury were “cut off”, meaning that the actual spinal cord (again, the main “highway”) itself was damaged and not just the spinal nerves.
How Did This Happen?: A lot of changes (in the rules, anyway) have been made in the NFL over the last several years in regards to tackling, and a lot of those changes have centered around limiting the times a player is allowed to make a helmet-to-helmet hit on another player. But, what people fail to mention most of the time is that these rules are not only beneficial to the player being hit, but they’re also beneficial to the player doing the hitting. It’s a lot like boxing gloves in the sense that most people think the gloves were put in place to protect the guy whose head is being punched (and yes, they do help him/her, too), when in reality the gloves were introduced to protect the punchers (relatively weak) bones in their hand to prevent them from breaking.
The NFL and youth football organizations such as USA Football have recently made strides to educate players, coaches and parents about the importance of “keeping your head up” while making a tackle, and here’s the science behind why it’s so important:
When the neck is in its “natural” position it has a (healthy) curvature to it, it’s not a “straight stack” (in doctor talk the cervical spine is said to be “extended as a result of normal cervical lordosis”). When the head is lowered (i.e. when the neck is flexed) about 30 degrees the cervical spine straightens, and that normal curvature is lost. Instead what you have now is a straight line (see figure below), and as it turns out loss of that natural curvature in the neck at the time of impact is crucialto leading to injury.

When players use proper tackling techniquethe cervical spine is able to effectively dissipate (“scatter”) a lot of the energy from the hit off into the muscles of the neck and shoulders, and some of that force can also be used to bend and flex the neck in ways that aren’t harmful to the body. However, when a player decides to “drop their head” to make a hit the curvature in the neck is replaced by a straight-line, and all of that energy that could have been scattered in all the ways we mentioned above, has to now be absorbed almost entirely by bones, the disks, and the ligaments in the neck. With the bones in the neck now stacked one on top of the other, the result is that the cervical spine is compressed between the rapidly moving head on one end, and the force of both the body it’s connected to and the one it’s about to smash into.
With nowhere for all of that energy to go, the straightened cervical spine buckles, and (as in Devon’s case) can break under the pressure. Now left unprotected, the soft spinal cord is susceptible to be being stretched, pinched, torn or even severed (see figure below).

Where To From Here?:Football is a violent game, period. And, there is no amount of Nerf in the world that is going to eliminate all football injuries, we know this. But, teaching the up and coming young players proper technique is one step in the right direction and we hope that by helping you have a better understanding of the science and anatomy behind it all that you’ll feel more confident to step in and correct a player, or even a coach, who is not doing his or her part to protect kids (or adults for that matter). As for those that take the ridiculous stance that all these rules are “making the game boring and soft”, here’s a prime example of a bigandexciting hit being made, all while using proper technique. But you want to know what is most impressive about the hit? Both players got right back up, and lined up to do it all again. Now that’sfootball!
Show Some Love, “Like” Us On: FaceBook
And Follow Us On Twitter: @Health_ID
“Some of y’all wont have sex without a condom. That’s good. But you’ll gladly go down on somebody? See…I don’t get it. Because now, you done ATE the disease.”
-Unknown Comedian
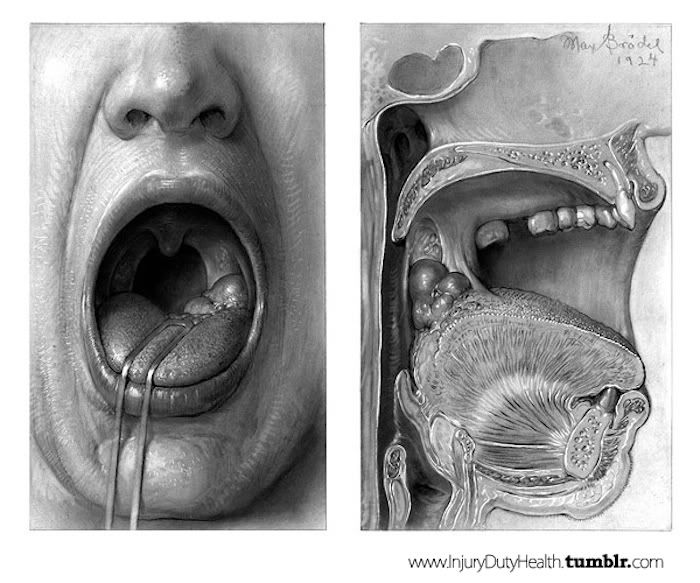
Get this, despite the recent drop in use of tobacco products, oral cancers (which include cancers of the tongue, tonsils and the back of the throat) are on the rise. This is a little surprising, because use of tobacco products has been the #1 cause of these cancers for a while now.
What’s behind the rise? The Human papillomavirus or HPV (a virus proven to be linked to cervical cancer in women). Yup, many scientists now believe that the growing popularity/practice of oral sex is behind the jump in the number of people developing oral cancer.
Steven Gill, Ph.D., associate professor of Microbiology and Immunology and a scientist in the Center for Oral Biology at the University of Rochester Medical Center School of Medicine and Dentistry in Up-State New York is the man behind some of the current research being done and he had this to say:
“It’s possible that pockets of gum inflammation and tissue destruction in the mouth provide a reservoir for HPV, which the virus uses to infect nearby tissue. Other teams are studying the link as well. Recently in the journal Archives of Otolaryngology, scientists describe a possible association between oral inflammatory disease – chronic periodontitis or gum disease – and HPV infection in patients with head and neck cancers.”
Foul Mouthed: We’re not trying to ruin your next kiss, but here is a not-so-cool-party-fact: There are more than 800 types of bacteria living in the space between your lips and your throat. And that’s no typo. 800. But here’s the thing, they’re actually not allbad. In fact, most of them are there keeping other potentially dangerous bacteria “in-check”.
What To Do About It: Researchers are in the middle of taking a closer look at the bacteria in the mouths of those with oral cancers and comparing the findings with the “healthier” mouths of those without oral cancer. The goal is to hopefully find which bacteria may actually play a role in the development of some types of cancer.
Now, we’re going to say this, even though most of you will likely ignore it: Dental Dam. Read about it, use it (…we figured we’d at least try). In the mean time Dr. Steven Gill, Ph.D., stresses the importance of preventing oral inflammatory disease as a key way for helping to prevent an HPV infection of your mouth. Brushing and flossing your grill regularly, are easy steps to fight gum disease and increase the likelihood that the HPV virus doesn’t have any easy openings to sneak in through, and that the “good bacteria” aren’t overtaken by the “bad ones” in your mouth and throat.
So, get to scrubbin’ before you get to lovin’!
 16 days until I make the second biggest (and fi")
Budapest, Hungary (by Gareth Bevan)
16 days until I make the second biggest (and first voluntary) move of my life.
Post link



T-143
I remember drawing all the branches of the abdominal aorta until its terminal branches back when I was a first year med student. Yet, I can’t seem to master them completely!
ig:studyingdoc


259 of 366
Going back to biochemistry basics this week really helped me understand the various clinical diseases I’ve encountered throughout med school :)
ig:studyingdoc


258 of 366(?)
I don’t even know if this countdown ‘til end kf internship still applies, but keeping it there for the sake of it.
Hey guys, it’s been 4 days since we, medical interns, were pulled out from the hospital because of the corona virus outbreak. Everything happened so fast. I was catching babies that day for my neonatal rotation, then hours later, I was on a car ride home to my province.
Here I am on my 4th day of quarantine. My sister recently developed fever, cough, and difficulty of breathing. She’s currently admitted in a hospital back in Manila and fortunately, she’s stable. Meanwhile I’ve had cough, colds, and malaise ever since I arrived. This is why I’m taking this self-quarantine seriously. I haven’t touched or hugged any family member ever since I arrived because I can’t risk exposing my parents (who are both >60 years old) if ever I did catch the virus.
Anyway, I have 10 days left. I’ve been using this time to study Biochemistry through online videos and books even though I’m not sure if we’re gonna be able to take the licensure exam this year. The future is so unclear, and that thought kinda makes me feel demotivated. But I try to brush it off, just try to study like I usually do.
I hope everyone’s okay at this time of crisis. I pray for everyone who can’t stay home because they have to earn for their families. I pray for our frontliners, and my co-interns who volunteered to stay in the hospita despite the pullout. It’s times like these that we really need to help each other. I pray that this will pass soon. :)
ig:studyingdoc

A bird explaining to a hedgehog crossing so it doesn’t die.
Senior residents @ me, circa every freaking year of med school and my residency