With public conversations about periods, pregnancy and the menopause at an all time high, it can sometimes feel like we’ve never been more aware of women’s health issues. But data exclusively seen by i suggests women are still worryingly clueless about their own bodies – and it could have serious consequences health consequences.
According to a YouGov survey carried out by gynaecological cancer charity The Eve Appeal, just 51 per cent of women can correctly label all five parts of their gynaecological anatomy on a diagram. Revisiting survey questions first put to the public in 2014, the Eve Appeal found some, but very little, improvement in women’s ability to identify the ovaries, womb, cervix, vagina and vulva on an anatomical diagram.
“Some of y’all wont have sex without a condom. That’s good. But you’ll gladly go down on somebody? See…I don’t get it. Because now, you done ATE the disease.”
-Unknown Comedian
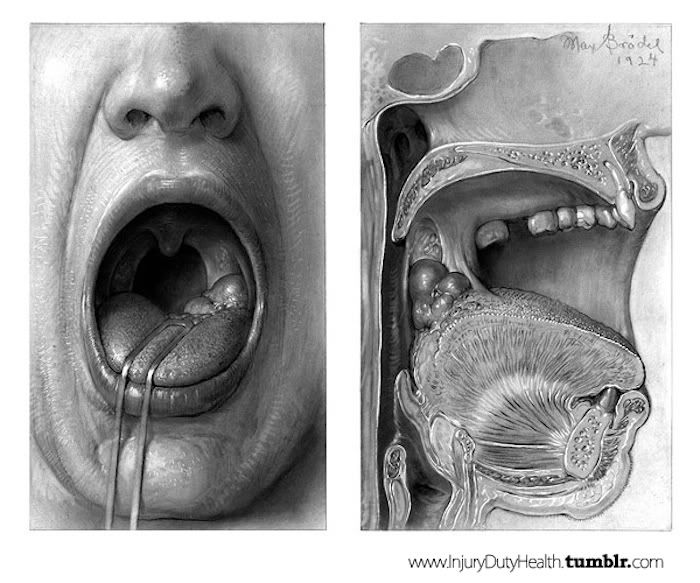
Get this, despite the recent drop in use of tobacco products, oral cancers (which include cancers of the tongue, tonsils and the back of the throat) are on the rise. This is a little surprising, because use of tobacco products has been the #1 cause of these cancers for a while now.
What’s behind the rise? The Human papillomavirus or HPV (a virus proven to be linked to cervical cancer in women). Yup, many scientists now believe that the growing popularity/practice of oral sex is behind the jump in the number of people developing oral cancer.
Steven Gill, Ph.D., associate professor of Microbiology and Immunology and a scientist in the Center for Oral Biology at the University of Rochester Medical Center School of Medicine and Dentistry in Up-State New York is the man behind some of the current research being done and he had this to say:
“It’s possible that pockets of gum inflammation and tissue destruction in the mouth provide a reservoir for HPV, which the virus uses to infect nearby tissue. Other teams are studying the link as well. Recently in the journal Archives of Otolaryngology, scientists describe a possible association between oral inflammatory disease – chronic periodontitis or gum disease – and HPV infection in patients with head and neck cancers.”
Foul Mouthed: We’re not trying to ruin your next kiss, but here is a not-so-cool-party-fact: There are more than 800 types of bacteria living in the space between your lips and your throat. And that’s no typo. 800. But here’s the thing, they’re actually not allbad. In fact, most of them are there keeping other potentially dangerous bacteria “in-check”.
What To Do About It: Researchers are in the middle of taking a closer look at the bacteria in the mouths of those with oral cancers and comparing the findings with the “healthier” mouths of those without oral cancer. The goal is to hopefully find which bacteria may actually play a role in the development of some types of cancer.
Now, we’re going to say this, even though most of you will likely ignore it: Dental Dam. Read about it, use it (…we figured we’d at least try). In the mean time Dr. Steven Gill, Ph.D., stresses the importance of preventing oral inflammatory disease as a key way for helping to prevent an HPV infection of your mouth. Brushing and flossing your grill regularly, are easy steps to fight gum disease and increase the likelihood that the HPV virus doesn’t have any easy openings to sneak in through, and that the “good bacteria” aren’t overtaken by the “bad ones” in your mouth and throat.
My soul sister and friend IRL Jenna Longoria (aka the Period Guru) is hosting a Masterclass for Period Solutions.
If you have painful periods or have been diagnosed with a period-related condition like endometriosis or PCOS, I highly recommend that you start following Jenna (@jennalongoriahealth on Instagram) and take this Master Class.
I have personally been working with her over the last 4 months with some of my hormone imbalances, and her awareness of all things hormones is unparalleled. I believe hormone health is something that is not well-understood or supported by standard medical practice, and much of the suffering is quite unnecessary. Jenna’s website is linked below.
Hope you are all in good spirits and undeterred by this current climate. Xoxo Nikki
I have been going through some health struggles, and it’s been extra hard for me because I really identify with being a person who prioritizes her health.
I have a lot of unhelpful thoughts about why or how or when, but I can think about it all I want, and it really doesn’t matter. All those thoughts are just either negative judgments about the situation or endless chatter that distract me from the task at hand.
When I reflect on it, I’m proud of myself. I accepted the situation, I learned a lot, I’ve asked for help, I’ve gone through a lot of healing and detox already…. I have realized that I have this attachment to “Healthy Person” ego identity. And I haven’t gone the other way to attach to the “Disease Warrior” ego identity either. That’s a lot of growth in the past few months.
Our bodies are both incredibly fragile, and startlingly resilient. I think we might look back in 100 years and wondered how we survived in this toxic mess we currently live in. I’m wondering that now. If you’re going through health troubles, I’m wishing you speedy acceptance, healing, and growth as a person.
I’m a witch who proudly and vehemently knows that women deserve control and power over their own body and the choices they make for themselves. If you disagree, then disrespectfully fuck off and burn.
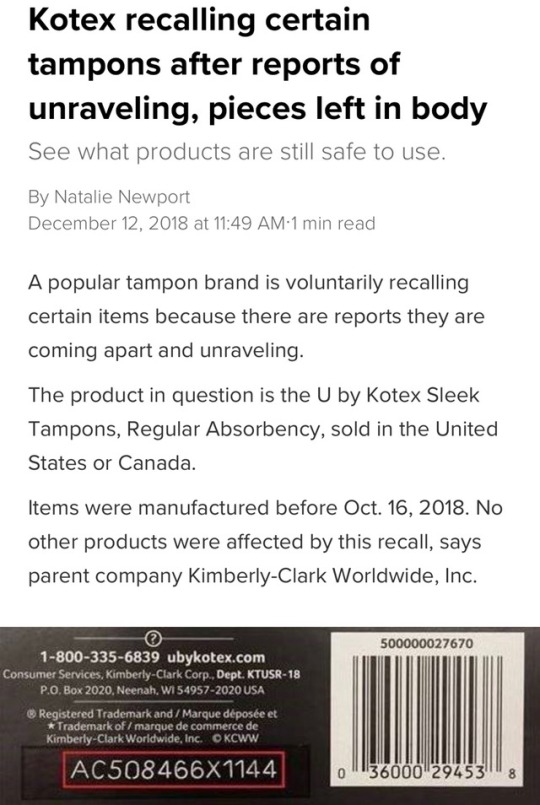
“The recall is limited to specific lots of U by Kotex® Sleek® Tampons, Regular Absorbency, that were manufactured between October 7, 2016 and October 16, 2018 and distributed between October 17, 2016 and October 23, 2018. Consumers can identify this product by looking for specific lot numbers found on the bottom of the package. A full list of recalled lot numbers is available on the U by Kotex® website. Retailers have been alerted to remove the recalled lot numbers from shelves and post a notification in their stores. “
MEMORIZE THE PACKAGING SO YOU MAKE SURE YOU NEVER BUY THIS CREAM FOR YOURSELF OR ANYONE YOU LOVE.
This post is about vaginas. My vagina in particular. I get yeast infections pretty regularly, and until recently I was able to afford to see a doctor who could prescribe me fluconazole.
Fluconazole, a drug also known by the brand name Diflucan, is a small pink pill. You take two pills a few days apart from each other to restore balance and harmony to your bountiful folds. I’ve never ever had a bad side effect from taking this pill.
Cut to November 2016. I’m a recent college grad without reliable health care coverage in the process of finding a job. And I’m dealing with a yeast infection. Before I moved out of state, my previous doctor told me about Miconazole. She said it was as effective as the pill and hallelujah, it’s over the counter! I decided to purchase the cream pictured above. This treatment only lasted 3 days, a convenient time frame for my schedule.
The application process was a little messy, and some of the cream came in contact with my vulva and labia. Within 5 minutes every piece of skin that had come in contact with the cream, excluding my hands, was on fire. I wanted to scream it was so painful. I began frantically searching for what I should do online.
I found a whole forum of people on drugs.com who had experienced something similar. These comments saved me, and these were just on the first page. There were 33 pages total, the earliest dated July 2009.
I was writhing in pain at 2AM when I found this forum (which I found by searching “my vagina burn itch hurts after miconazole” on Google). As soon as I read these comments I threw the devil cream directly into the trash and jumped in the shower. I didn’t feel any actual relief until I reached in and scraped the cream out of me. I paid $17 plus tax on this bullshit, but I could have just as easily ripped up my money or paid someone to not hurt me.
The moral of the story is that vaginal health care is is completely fucked up because we don’t have access to an over the counter cure for yeast infections that is safe for our bodies and also YOU SHOULD NEVER BUY THIS CREAM EVER.
Reblog to save a vagina.
Okay so I used to get yeast infections every month after my period ‘cause my pH levels were fucked up or something (idk that’s what my doctor said) and I actually used to take this stuff and it was fine. Then a couple years down the road I had a yeast infection for the first time in ages and I used this again and it burned so bad I had to sit in the bath and like physically dig it out of my vagina
AND THEN I LEARNED THAT IT’S BECAUSE I DIDN’T HAVE A YEAST INFECTION. I had a bacterial infection, which is honestly pretty much identical to a yeast infection depending on the severity. The only difference is that IF YOU HAVE A BACTERIAL INFECTION AND TRY TO USE YEAST INFECTION MEDICATION IT WILL HURT
But it’s not actually the medication’s fault. The medication DOES do what it’s supposed to do, provided you’re actuallysuffering from a yeast infection. Chances are though that you and every one who commented on this did, in fact, have bacterial infections instead.
FORTUNATELY they also make over the counter tests so you can know if you need to call your doctor or just grab some yeast medicine off the shelf. Next time if you aren’t sure, pee on a stick and save yourself a world of fucking pain
AMEN.
It’s unfortunate that I’m 27 and never knew that last bit of information. The world of vaginal health is so obscure and inaccessible.
Same. I know I have BV, and I’ve bought litmus paper from American Science & Surplus, but it’s nice to know there’s something I can get at the drugstore.
I was so worried when i read the original post! Here’s more info.
1) Yeast infection creams DO WORK! Especially if you have a bad one. For a yeastie that’s mild or just coming on, you can also try a garlic clove in the vag, changing every 12 hours. It works as an anti-fungal. Be sure to cut down on sugar in your diet if you’re getting yeast infections. Sugar is what candida eats, it’s like adding gasoline to the fire.
2) But before any of those things, be sure it’s actually a yeast infection first. Reading those reviews breaks my heart! Putting creams in there with a bacterial infection will definitely irritate it. Yeast infections can look a lot like BV, trichomoniasis, or chlamydia:
You can figure out what’s up with a home kit. Yes, it’s another 15 bucks or so (for 2), but if you’re skipping the doctor it is necessary! If you actually have a bacterial infection and leave it untreated, it will not only hurt but make you more susceptible to STIs, scarring, and even infertility. FYI, these kits also exist for UTIs which can also easily be mistaken for other types of infection.
I have never in my life been so angry at a commercial as I am at this commercial. Who invented this shit Mitch McConnell? Now we get to punish ourselves, before, during AND after we have that dirty dirty sex.
(1) Abortion services are essential to health care and access to those services is central to people’s ability to participate equally in the economic and social life of the United States. Abortion access allows people who are pregnant to make their own decisions about their pregnancies, their families, and their lives.
(2) Since 1973, the Supreme Court repeatedly has recognized the constitutional right to terminate a pregnancy before fetal viability, and to terminate a pregnancy after fetal viability where it is necessary, in the good-faith medical judgment of the treating health care professional, for the preservation of the life or health of the person who is pregnant.
(3) Nonetheless, access to abortion services has been obstructed across the United States in various ways, including blockades of health care facilities and associated violence, prohibitions of, and restrictions on, insurance coverage; parental involvement laws (notification and consent); restrictions that shame and stigmatize people seeking abortion services; and medically unnecessary regulations that neither confer any health benefit nor further the safety of abortion services, but which harm people by delaying, complicating access to, and reducing the availability of, abortion services.
(4) Reproductive justice requires every individual to have the right to make their own decisions about having children regardless of their circumstances and without interference and discrimination. Reproductive Justice is a human right that can and will be achieved when all people, regardless of actual or perceived race, color, national origin, immigration status, sex (including gender identity, sex stereotyping, or sexual orientation), age, or disability status have the economic, social, and political power and resources to define and make decisions about their bodies, health, sexuality, families, and communities in all areas of their lives, with dignity and self-determination.
(5) Reproductive justice seeks to address restrictions on reproductive health, including abortion, that perpetuate systems of oppression, lack of bodily autonomy, white supremacy, and anti-Black racism. This violent legacy has manifested in policies including enslavement, rape, and experimentation on Black women; forced sterilizations; medical experimentation on low-income women’s reproductive systems; and the forcible removal of Indigenous children. Access to equitable reproductive health care, including abortion services, has always been deficient in the United States for Black, Indigenous, and other People of Color (BIPOC) and their families.
(6) The legacy of restrictions on reproductive health, rights, and justice is not a dated vestige of a dark history. Presently, the harms of abortion-specific restrictions fall especially heavily on people with low incomes, BIPOC, immigrants, young people, people with disabilities, and those living in rural and other medically underserved areas. Abortion-specific restrictions are even more compounded by the ongoing criminalization of people who are pregnant, including those who are incarcerated, living with HIV, or with substance-use disorders. These communities already experience health disparities due to social, political, and environmental inequities, and restrictions on abortion services exacerbate these harms. Removing medically unjustified restrictions on abortion services would constitute one important step on the path toward realizing Reproductive Justice by ensuring that the full range of reproductive health care is accessible to all who need it.
(7) Abortion-specific restrictions are a tool of gender oppression, as they target health care services that are used primarily by women. These paternalistic restrictions rely on and reinforce harmful stereotypes about gender roles, women’s decision-making, and women’s need for protection instead of support, undermining their ability to control their own lives and well-being. These restrictions harm the basic autonomy, dignity, and equality of women, and their ability to participate in the social and economic life of the Nation.
(8) The terms “woman” and “women” are used in this bill to reflect the identity of the majority of people targeted and affected by restrictions on abortion services, and to address squarely the targeted restrictions on abortion, which are rooted in misogyny. However, access to abortion services is critical to the health of every person capable of becoming pregnant. This Act is intended to protect all people with the capacity for pregnancy—cisgender women, transgender men, non-binary individuals, those who identify with a different gender, and others—who are unjustly harmed by restrictions on abortion services.
(9) Since 2011, States and local governments have passed nearly 500 restrictions singling out health care providers who offer abortion services, interfering with their ability to provide those services and the patients’ ability to obtain those services.
(10) Many State and local governments have imposed restrictions on the provision of abortion services that are neither evidence-based nor generally applicable to the medical profession or to other medically comparable outpatient gynecological procedures, such as endometrial ablations, dilation and curettage for reasons other than abortion, hysteroscopies, loop electrosurgical excision procedures, or other analogous non-gynecological procedures performed in similar outpatient settings including vasectomy, sigmoidoscopy, and colonoscopy.
(11) Abortion is essential health care and one of the safest medical procedures in the United States. An independent, comprehensive review of the state of science on the safety and quality of abortion services, published by the National Academies of Sciences, Engineering, and Medicine in 2018, found that abortion in the United States is safe and effective and that the biggest threats to the quality of abortion services in the United States are State regulations that create barriers to care. These abortion-specific restrictions conflict with medical standards and are not supported by the recommendations and guidelines issued by leading reproductive health care professional organizations including the American College of Obstetricians and Gynecologists, the Society of Family Planning, the National Abortion Federation, the World Health Organization, and others.
(12) Many abortion-specific restrictions do not confer any health or safety benefits on the patient. Instead, these restrictions have the purpose and effect of unduly burdening people’s personal and private medical decisions to end their pregnancies by making access to abortion services more difficult, invasive, and costly, often forcing people to travel significant distances and make multiple unnecessary visits to the provider, and in some cases, foreclosing the option altogether. For example, a 2018 report from the University of California San Francisco’s Advancing New Standards in Reproductive Health research group found that in 27 cities across the United States, people have to travel more than 100 miles in any direction to reach an abortion provider.
(13) An overwhelming majority of abortions in the United States are provided in clinics, not hospitals, but the large majority of counties throughout the United States have no clinics that provide abortion.
(14) These restrictions additionally harm people’s health by reducing access not only to abortion services but also to other essential health care services offered by many of the providers targeted by the restrictions, including—
(A) screenings and preventive services, including contraceptive services;
(B) testing and treatment for sexually transmitted infections;
(D) referrals for primary care, intimate partner violence prevention, prenatal care and adoption services.
(15) The cumulative effect of these numerous restrictions has been to severely limit the availability of abortion services in some areas, creating a patchwork system where access to abortion services is more available in some States than in others. A 2019 report from the Government Accountability Office examining State Medicaid compliance with abortion coverage requirements analyzed seven key challenges (identified both by health care providers and research literature) and their effect on abortion access, and found that access to abortion services varied across the States and even within a State.
(16) International human rights law recognizes that access to abortion is intrinsically linked to the rights to life, health, equality and non-discrimination, privacy, and freedom from ill-treatment. United Nations (UN) human rights treaty monitoring bodies have found that legal abortion services, like other reproductive health care services, must be available, accessible, affordable, acceptable, and of good quality. UN human rights treaty bodies have likewise condemned medically unnecessary barriers to abortion services, including mandatory waiting periods, biased counseling requirements, and third-party authorization requirements.
(17) Core human rights treaties ratified by the United States protect access to abortion. For example, in 2018, the UN Human Rights Committee, which oversees implementation of the ICCPR, made clear that the right to life, enshrined in Article 6 of the ICCPR, at a minimum requires governments to provide safe, legal, and effective access to abortion where a person’s life and health is at risk, or when carrying a pregnancy to term would cause substantial pain or suffering. The Committee stated that governments must not impose restrictions on abortion which subject women and girls to physical or mental pain or suffering, discriminate against them, arbitrarily interfere with their privacy, or place them at risk of undertaking unsafe abortions. Furthermore, the Committee stated that governments should remove existing barriers that deny effective access to safe and legal abortion, refrain from introducing new barriers to abortion, and prevent the stigmatization of those seeking abortion.
(18) UN independent human rights experts have expressed particular concern about barriers to abortion services in the United States. For example, at the conclusion of his 2017 visit to the United States, the UN Special Rapporteur on extreme poverty and human rights noted concern that low-income women face legal and practical obstacles to exercising their constitutional right to access abortion services, trapping many women in cycles of poverty. Similarly, in May 2020, the UN Working Group on discrimination against women and girls, along with other human rights experts, expressed concern that some states had manipulated the COVID–19 crisis to restrict access to abortion, which the experts recognized as “the latest example illustrating a pattern of restrictions and retrogressions in access to legal abortion care across the country” and reminded U.S. authorities that abortion care constitutes essential health care that must remain available during and after the pandemic. They noted that barriers to abortion access exacerbate systemic inequalities and cause particular harm to marginalized communities, including low-income people, people of color, immigrants, people with disabilities, and LGBTQ people.
(19) Abortion-specific restrictions affect the cost and availability of abortion services, and the settings in which abortion services are delivered. People travel across State lines and otherwise engage in interstate commerce to access this essential medical care, and more would be forced to do so absent this Act. Likewise, health care providers travel across State lines and otherwise engage in interstate commerce in order to provide abortion services to patients, and more would be forced to do so absent this Act.
(20) Health care providers engage in a form of economic and commercial activity when they provide abortion services, and there is an interstate market for abortion services.
(21) Abortion restrictions substantially affect interstate commerce in numerous ways. For example, to provide abortion services, health care providers engage in interstate commerce to purchase medicine, medical equipment, and other necessary goods and services. To provide and assist others in providing abortion services, health care providers engage in interstate commerce to obtain and provide training. To provide abortion services, health care providers employ and obtain commercial services from doctors, nurses, and other personnel who engage in interstate commerce and travel across State lines.
(22) It is difficult and time and resource-consuming for clinics to challenge State laws that burden or impede abortion services. Litigation that blocks one abortion restriction may not prevent a State from adopting other similarly burdensome abortion restrictions or using different methods to burden or impede abortion services. There is a history and pattern of States passing successive and different laws that unduly burden abortion services.
(23) When a health care provider ceases providing abortion services as a result of burdensome and medically unnecessary regulations, it is often difficult or impossible for that health care provider to recommence providing those abortion services, and difficult or impossible for other health care providers to provide abortion services that restore or replace the ceased abortion services.
(24) Health care providers are subject to license laws in various jurisdictions, which are not affected by this Act except as provided in this Act.
(25) Congress has the authority to enact this Act to protect abortion services pursuant to—
(A) its powers under the commerce clause of section 8 of article I of the Constitution of the United States;
(B) its powers under section 5 of the Fourteenth Amendment to the Constitution of the United States to enforce the provisions of section 1 of the Fourteenth Amendment; and
(26) Congress has used its authority in the past to protect access to abortion services and health care providers’ ability to provide abortion services. In the early 1990s, protests and blockades at health care facilities where abortion services were provided, and associated violence, increased dramatically and reached crisis level, requiring Congressional action. Congress passed the Freedom of Access to Clinic Entrances Act (Public Law 103–259; 108 Stat. 694) to address that situation and protect physical access to abortion services.
(27) Congressional action is necessary to put an end to harmful restrictions, to federally protect access to abortion services for everyone regardless of where they live, and to protect the ability of health care providers to provide these services in a safe and accessible manner.
(b) Purpose.—It is the purpose of this Act—
(1) to permit health care providers to provide abortion services without limitations or requirements that single out the provision of abortion services for restrictions that are more burdensome than those restrictions imposed on medically comparable procedures, do not significantly advance reproductive health or the safety of abortion services, and make abortion services more difficult to access;
(2) to promote access to abortion services and women’s ability to participate equally in the economic and social life of the United States; and
(3) to invoke Congressional authority, including the powers of Congress under the commerce clause of section 8 of article I of the Constitution of the United States, its powers under section 5 of the Fourteenth Amendment to the Constitution of the United States to enforce the provisions of section 1 of the Fourteenth Amendment, and its powers under the necessary and proper clause of section 8 of article I of the Constitution of the United States.
So, the Australian government today announced, that they are abolishing the piss poor replacement piece of shit body that governs infant formula marketing.
The marketing code in Australia only covered infant formula up to 12 months, so “Toddler formula” with the exact same branding and messaging as infant formula was created. But at least there was something..
So far, there’s nothing that will replace APMAIF. Tony Abbott is once again a huge fucknuckle of a syphillitic scrotum, who believes that anyone who is not rich as fuck white man (or one of the women he owns) is not worthy of any government spending.
Now, there will literally be nothing to stop unethical marketing to persuade new parents who are extra vulnerable to marketing to buy their brand of formula. Nothing to make sure that if extra ingredients in infant formula are beneficial for babys development, that they are put in ALL infant formulae, and not just the premium priced ones.
Nothing to stop unethical marketing practices that serve to convince new parents that they should doubt the lactation process without good reason. Nothing to stop infant formula and baby food manufacturers from encouraging parents to introduce foods in ways that might be damaging to their baby even though it lines the pockets of the greedy rich fucks.
Because we are total nerds, Testosterone boasts a molecular model beard and Estrogen is sporting the molecular structure for estradiol, one of three types of estrogen made by humans. We especially love the beautiful form of the amino acid chain that comprises Insulin.
The federal government has issued new rules aimed at eliminating systemic gender bias in medical research. It’s no longer enough for scientists testing drugs and doing other kinds of research to include women in clinical studies at the end of the process, the National Institutes of Health says. From now on, scientists must begin using female subjects in their very first laboratory experiments — including female animals and female-derived cells.
Researchers [have often] avoided using female animals for fear that their reproductive cycles and hormone fluctuations would confound the results of delicately calibrated experiments.
That laboratory tradition has had enormous consequences for women. Name a new drug or treatment, and odds are researchers know far more about its effect on men than on women.
It’s been 25 years or so since gender bias in medical studies emerged as a major women’s health issue. Women now make up more than half the participants in government-funded clinical research, but they are still often underrepresented in clinical trials carried out by private companies.
Partly as a result, women experience more severe side effects from new treatments, studies have shown.
Yet clinical studies are just the last stage of the lengthy process of developing drugs and medical devices. And even in NIH-funded studies, female subjects continue to be hugely underrepresented in earlier stages of lab research, Roni Caryn Rabin reports.
Bias in mammalian test subjects was evident in eight of 10 scientific disciplines in an analysis of published research conducted by Irving Zucker, a professor of psychology and integrative biology at the University of California, Berkeley. The most lopsided was neuroscience, where single-sex studies of male animals outnumbered those of females by 5.5 to 1.
Even when researchers study diseases that are more prevalent in women — including anxiety, depression, thyroid disease and multiple sclerosis — they often rely on male animals, Zucker has found.
Today’s heroin users are more likely to be female than in the 1960s,vox’s German Lopez reports.They’re also older and much whiter than in the past, and much more likely to have gotten hooked first on prescription drugs.
Data from a new retrospective analysis by researchers at Washington University in St. Louis and Nova Southeastern University in Miami, published in JAMA Psychiatry.
More and more laws have been restricting and banning abortions across the U.S., here’s what’s happening and what you can do about it.
What happened in Alabama?
Tuesday, Alabama’s state senate passed a ban on abortion, making it a crime for doctors to perform the procedure, at any stage of pregnancy.
Doctors could face up to 99 years in prison for helping their patients terminate unwanted or unviable pregnancies.
This law was decided on by 25 white men, and passed by a vote of 25 vs 6. The 3 women on the state senate all voted against it. However, the law was written, and signed, by two women.
These senators refused to add exceptions for cases of rape or incest, by voting against democratic amendments. The text only allows an exception when the pregnant woman’s health is at serious risk. This gives women lesser rights than those of rapists or abusers, and makes the abortion ban the strictest in the US.
Wednesday, Alabama’s Republican governor, Kay Ivey, signed it into law.
This does not immediately outlaw the procedure (which is currently still legal). The measure would take effect in six months, if it passes.
These anti-abortion politicians want to overturn Roe v Wade, the landmark ruling that legalized abortion nationwide in 1973, by taking this ban to the supreme court. In other words, they’re working to make abortions illegal across the country. So, if you think this bill doesn’t concern you, IT DOES.
Alabama is one of 16 (Republican controlled) states to introduce or pass anti-abortion laws. This represents a growing push against women’s reproductive rights in the U.S., fuelled by right-wing, republican Christians, and made worse under Trump’s presidency.
What are we doing to stop this?
State senator Vivian Davis Figures fought hard against this bill. She told the male lawmakers: “You don’t have to raise that child. You don’t have to carry that child. You don’t have to do anything for that child, but you want to make the decision for that woman.” She proposed amendments to expand Medicaid, force legislators who voted for the measure to pay the state’s legal bills, or make it a crime for men to get vasectomies. All were rejected.
Pro-choice activists have promised to challenge the measure in court. The ACLU said it will file a lawsuit (with Planned Parenthood) “to stop this unconstitutional ban and protect every woman’s right to make her own choice about her healthcare, her body and her future.” The legal battle could stop the restrictions entirely, or at least delay them.
They also acted against the spread of fear and misinformation. Staci Fox, CEO of Planned Parenthood Southeast Advocates, stressed that abortion is currently still legal in all 50 states. And the ACLU of Alabamatweeted “PLEASE REMEMBER: This bill will not take effect anytime in the near future, and abortion will remain a safe, legal medical procedure at all clinics in Alabama.” Don’t forget to also share this message for people who might need to read it.
The Yellow Hammer Fund, which helps patients seeking care at one of Alabama’s 3 abortion clinics.
The Abortion Funds, which gives patients facing financial and logistical barriers access to safe abortions.
Emily’s list, which gets pro-choice Democratic women elected to office.
The Democratic Party, which pledged to “protect a woman’s right to safe and legal abortion".
Here are some more things you can do right now:
You can participate in the online donation campaignDemocrat senator Cory Booker created to help some of the organizations listed above to protect access to abortions.
You can check and share this Twitter thread to know which organizations help provide safe abortions near you.
You can write to Alabama’s Governor Kay Ivey via Planned Parenthood, here.
Also, if you’re from Alabama, support and vote for Vivian Davis Figures, who fought this bill in her state senate, pledged to “continue to stand for the rights of ALL women to use our God given free will”, and is running for re-election in early June.
Please share any additional information or ressources, and spread this shit like wildfire.
Women with diabetes need comprehensive care before and during pregnancy. The Diabetes and Pregnancy Program (DAPP) at UC San Diego Health, the only one of its kind in the San Diego Region, cares for the diverse population of women with diabetes in San Diego County.
DAPP is designed to provide specialized care to patients with diabetes through a multidisciplinary approach, following the California Diabetes and Pregnancy Program guidelines.
“Patients with type 1 or type 2 diabetes, or those who have recently been diagnosed with gestational diabetes, require a team of specialists to assist with a healthy pregnancy and optimize the outcome for both the patient and baby,” said Sandy Ramos, MD, director of DAPP and perinatologist at UC San Diego Health.
“For example, working with a specialist to manage blood sugar before and during pregnancy can decrease the risk of complications and make it more likely that the patient can carry the baby to term.”
Question: How common is gestational diabetes and what are the complications?
Answer: Approximately one in five women delivering babies in San Diego County begin their pregnancies with diabetes, and others develop gestational diabetes during pregnancy. These women are at risk for complications during pregnancy and after delivery, including high blood pressure, eye disease, kidney disease, too much weight gain, severe hypoglycemia (low blood sugar) and diabetic ketoacidosis (DKA).
Their babies are also at increased risk for complications, including macrosomia (high birth weight), higher rates of miscarriage and stillbirth, birth defects, delivery complications and jaundice.
Q: What type of services does DAPP provide?
A: DAPP includes six certified diabetes care and education specialists (DECS), nutritionists and social workers under the direction of two maternal fetal medicine experts. The program provides care to approximately 500 patients with gestational diabetes, 120 patients with type 2 diabetes and 40 patients with type 1 diabetes per year.
As a clinical program in the region’s only academic medical center, DAPP provides leading edge diabetes care from preconception to postpartum, utilizing the latest technology available, including the use of sophisticated insulin pumps and continuous glucose monitoring.
For example, the DAPP team has found success using “closed loop systems” to improve glucose control in patients with type 1 diabetes in pregnancy. This technology allows integration of information from the continuous glucose monitor to augment or “talk” to insulin pumps. This allows the insulin pump to increase insulin delivery if the glucose values are high or to decrease or even suspend insulin delivery if the glucose value is low.
With the aim of improving the maternal and neonatal outcomes of women with diabetes, patients are also given the opportunity to participate in clinical trials, such as the Medical Optimization of Management of Pregnancy with Overt Diabetes (MOMPOD) trial, a randomized clinical trial of Metformin as an adjunct to insulin for the treatment of type 2 diabetes.
DAPP provides primary obstetrical care for complicated patients with diabetes and is able to provide consultative services to co-manage patients with gestational diabetes.
Q: How are you addressing gestational diabetes with patients in terms of lifestyle interventions and medications available?
A: To treat gestational diabetes, we encourage nutrition changes to limit simple carbohydrates and recommend exercise. Most patients with gestational diabetes can manage their glucose values with these changes alone. If elevations persist, they can be treated with medicines like insulin and metformin. However, these lifestyle changes are important tools to continue to lower the risk of development of type 2 diabetes. Women who develop gestational diabetes have a higher risk of developing type 2 diabetes later in life.
Q: What research needs to be done to improve how diabetes is managed in pregnancy?
A: There are many new medications used for management of type 2 diabetes that haven’t been studied in pregnancy. The issue of safety of these medications needs further exploration in pregnancy. Additionally, technology, including blue tooth-enabled meters and continuous glucose monitors, commonly used in type 1 diabetes, need to be studied in other types of diabetes in pregnancy to see if they may be useful tools to improve the care of women with diabetes.
A type of breast implant used by millions of women around the world is under scrutiny after French surgeons were advised to stop using it because of a potential link with a rare kind of cancer.
Textured breast implants have been linked with anaplastic large cell lymphoma (ALCL), which forms in the scar capsule around the implant and normally begins with pain and swelling in the breast.
Women who have the implants and capsules removed can make a full recovery, but if left untreated the disease can spread throughout the body and become life-threatening.
There is growing concern about the effects of the implants, with figures collected by plastic surgeons suggesting there have been at least 615 cases of the disease associated with breast implants, and 16 deaths.