In order to better understand cardiac defects, it’s best to start off reviewing how a normal heart works. First, the Superior and Inferior Vena Cava carrydeoxygenated blood into the heart (Right Atrium) from other parts of the body. The deoxygenated blood then passes through the TricuspidValve into the Right Ventricle. Thedeoxygenated blood is following the pathway through the heart in order to get to the lungs to gain oxygen, next the blood passes through the PulmonaryValveand enters the Pulmonary Artery, the pulmonary artery is special because it is the only artery in the body that carries deoxygenated blood. Once the deoxygenated blood passes through to theLungsit becomes oxygenated. The newly oxygenated blood then flows back to the heart through the Pulmonary Veins and into the Left Atrium. It then passes through the MitralValveand into the Left Ventricle. The blood is then contracted through the AorticValveinto the Aortaand to the rest of the body.
The Fetal Heart: During the fetal period and some time after birth, the circulation is quite different. The heart has more, holes, if you will in order for the fetal blood to bypass the lungs that are unable to oxygenate blood while the fetus is in utero. - The Foramen Ovale is an opening that allows passage of blood from the Right Atrium directly into the Left Atrium. The blood passing through is already oxygenated from the placenta. - The Ductus Arteriosus is an opening that passes oxygenated blood from the Pulmonary Artery directly into the Aortato get pumped to the rest of the body.
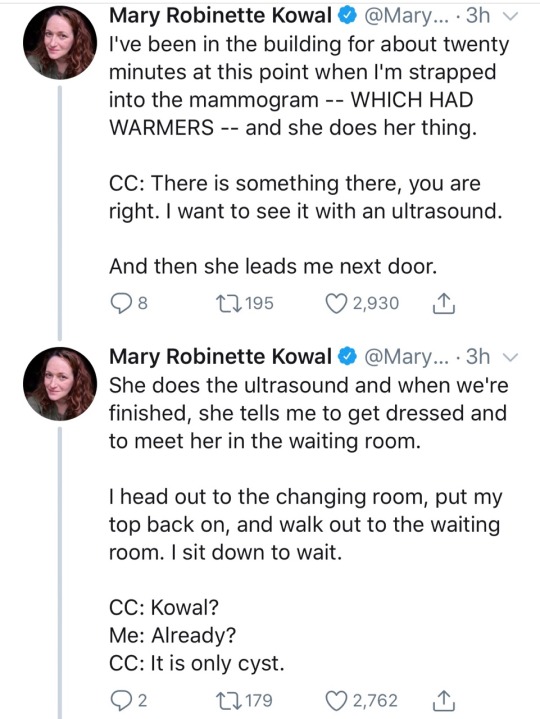
I was ramped up to 20-minute appointments last Friday and I am Not Okay. It is nearly 10pm and I only just finished my last chart note of the day about five minutes ago.
My documentation is suffering. My actual visits are suffering too: I’m missing important/worrisome shit because I’m so Fixated on finding a solution to the chief complaint that I’m overlooking high blood pressure readings and GAD-7 scores. I have one patient who I need to call first thing in the morning tomorrow because a couple of her PHQ-9 responses were Rather Worrying and I didn’t fucking notice until I was at home finishing her note. And I feel AWFUL about that.
If you ever feel like your healthcare provider is in a hurry, it’s because we are. And we absolutely hate it.
its pretty fucked up how many healthcare workers hate addicts, mentally ill people, and disabled people. did you think the job was just going to be patching up John Sports after the Big Game and looking after 8 year olds with broken arms?
A lot of people in the US are super worried about the Supreme Court axing Roe v. Wade, but what they might not know is that some states have laws in place that will protect the right to reproductive choice and abortion if that happens. One of these states is the state of Illinois. In 2019, a law was passed that protects abortion rights within the state even if the federal right to an abortion falls. This means that if Roe v. Wade is overturned, abortion will still be a protected right in Illinois. Even before Roe, Chicago was a haven for safe abortions- you just called and asked for Jane.
Now, safe abortion access is the law of the land in IL, and there are several groups who can help you. This post is long, but I think it’s worthwhile. Even if you don’t read all the way through it, maybe save it for later. You or someone you know might need it. If you want to stop now, the TL;DR is this:
f you’re a minor and you can’t tell your parents, get a waiver of notification from the IL Judicial Bypass program.
Schedule your appointment.
Contact abortion funds to get financial aid. Your home state might have s fund, and the Chicago Abortion Fund can help.
Secure housing for the procedure through the Midwest Access Coalition or by talking to the intake staff at the clinic of your choice.
I’d like to start by saying that the closer to home you get your abortion, should you need one, the easier it will be for you… probably. It depends on your individual situation AND your safety. If I still lived in Indiana and I needed an abortion, I’d probably leave to get it done, even though there are abortion providers in Indiana, because Indiana is super hostile and there’s lots of clinic protestors- for example, when I was taking my GRE my senior year at Notre Dame, the testing center was in this little strip mall in Mishawaka next to Planned Parenthood. Despite the fact that the PP in Mishawaka does not provide abortions, there were protestors who yelled at me for going in there. I wasn’t even going to PP. I’d like to say that I said something devastatingly cool but I just ran in flustered. Point being: It really, really would have sucked if I was there for healthcare instead of a standardized test for graduate school. And that’s a very tame, mild situation! Real abortion clinic protests are often much more devastating!
ANYWAYS. The less you have to travel, the easier things tend to be, if it’s safe to get an abortion where you are and if your state will have protected abortions if Roe is overturned. If you’re not sure what might happen in your state in that case, this map has a clear, succinct overview of the legal status of abortion in each state and all US territories. You will want to click through to that link, because this image isn’t interactive.
[ID: a map of the US with states and territories sorted by their legal protections for abortion into four categories: expanded access in the case of Roe v. Wade being overturned, protected, not protected, and hostile. IL is highlighted.]
So let’s say you live in any of those red states. (Yellow and blue are safe- abortion access is protected there.) Let’s say, worst case scenario, Roe gets overturned and you get pregnant and you want to terminate. You will be able to do that in IL, and it’s relatively easy to do that in Chicago for a relatively low cost and with the benefit of a robust support network of people who want to reaffirm your reproductive choices.
First, if you’re a minor and you don’t want to tell your parents because it’s not safe for you to do so, get a judicial waiver of parental notification. The IL ACLU has a judicial bypass hotline. This will come at no cost to you. Do this ASAP, because it takes time to get it set up! You can do this by calling the hotline at 877-442-9727, texting 312-560-6607, or emailing [email protected].
Next, you need to get an appointment set up. You could get a referral from someone local to you, but this can be tricky- 87% of counties in the US don’t have an abortion provider, and google can lead you to a crisis pregnancy center. They will not help you. If you have a local Planned Parenthood, call them. Even if they don’t provide abortions, they can refer you to someone who can. If you’re coming to Chicago, which this post… kind of assumes you are… you can call any of these groups to talk about your options and what clinics can help you. I recommend starting with FPA or PP; those are two actual clinics. MAC and CAF are funds- they can direct you but they can’t schedule an appointment for you.
You might want to shop around and see which clinic costs the least, and is the most practical for you to get to. FPA has a lot of patient resources, as does PP. Don’t be afraid to ask for financial assistance. The people staffing those organizations have extensive networks and deep compassion for their patients- if the clinic can’t help, they might know who can.
Once you’ve made an appointment, now’s the time to start gathering financial aid. Some insurance, including IL Medicaid, covers it. If yours does not, or if the copay is still too much, this is where abortion funds come into play. Many states have their own abortion funds for state residents, so you might have to look around to see who can help you. I’d start with the National Network of Abortion Funds.
You also need to figure out transportation and housing while you’re in the city to get your abortion. This isn’t super necessary if you’re just coming for the pill abortion, but if you’re coming for a d and c or other surgical procedure, you will be staying for a couple of days. THIS is why I’m writing this up, because abortion funds typically only are able to help cover the financial cost of the procedure. It’s expensive to stay somewhere and it can be absolutely terrifying if you’re on your own! Navigating while you’re in pain from the procedure can be an absolute devil of a time, too! However, Chicago has MAC (contact info above), which is a practicalaccess fund, which means that they help pay for transportation to the city (bus tickets and train tickets) and around the city (volunteer drivers or volunteers who take rideshares with clients), food, aftercare medicine (painkillers, etc.), and housing, and there’s also free access to emotional support staff throughout your stay. This is not just open to IL residents; it’s open to anyone coming to the city for an abortion. ALSO if you go through FPA, they have a partnership with the Hampton Inn a block away from their location where their patients get a discount. If you go that route, just talk to FPA about housing and they’ll hook you up. This can be super helpful if you need some evidence that you’re on a “business trip” or something like that- if you are in a position where you need an excuse for your safety, that might work well.
Hopefully you won’t need this post- but if you do, I hope it helps. Feel free to share it around. If you have anti-choice opinions and you feel the need to share, don’t. This isn’t the space for it; you will be blocked and your comments removed. And then remember that criminalizing abortion won’t stop abortion. It’ll just stop safe abortions. Also, increased access to abortion, funnily enough, tends to be the thing that lowers abortion rates, because increased access to abortion comes part and parcel with increased access to birth control and general health and sex education.
Reblogging this because it’s always relevant… and because an administrative decision by MAC’s incredible leadership means they don’t just do bus and train tickets anymore. They will also help pay for airline tickets if you need to fly. If you are in the US and need to come to Chicago for an abortion, MAC’s got your back.
Also, if you find yourself in a situation where you can’t travel, and you catch it early, you can do a medication abortion at home. This can either be clinician supported through telehealth or it can be a self-managed abortion (SMA). Either way, you can do this entirely online without ever having to go into a doctor’s office or clinic.
Now, this only works early in a pregnancy (up to 11-12 weeks), so if you’re in a situation where you suspect you may become pregnant and you don’t want to be, test early and often if you can. The various help lines can also help you figure out how far along you are.
More resources: https://www.reprolegalhelpline.org/- this link is a good resource for talking about your legal options. If you’re a pregnant person of color, immigrant, or low-income (and using Medicaid) in an abortion-hostile state, I HIGHLY recommend talking through your legal options because you are absolutely targeted by politicians and the US legal system.
You can print these on sticker paper at home if you have it. It’s a good way to get the word out.
As of… thirty minutes ago on Monday, 2 May 2022, Politico got hold of Justice Alito’s draft statement on Roe. It’s not good. We’re probably gonna lose Roe vs. Wade in two months, and that means if you live in a red state, you’re VERY probably going to lose the right to a safe abortion.
I know this is a long post, but if Roe is overturned, it’s not going to stop abortions. It’s just going to stop safe abortions. Abortion access is reproductive healthcare, and a lot of states are going to get really restrictive. Indiana, my home state, has already put a woman in jail for having a miscarriage. Oklahoma lawmakers would rather let women with ectopic pregnancies die than allow lifesaving medical procedures. This is bad, but! Underground abortion networks did exist before Roe vs. Wade, and now we have the internet. We have robust networks in place to help people that the government would rather see dead or imprisoned. Even if Roe is overturned, some states will be safe havens for abortion. Travel to these states can be difficult, but not impossible– that’s what abortion networks and abortion funds are for.
Please save as much of this information as may be relevant to you. And if you’re “pro-life” and feel the need to comment on this post? Don’t. Your opinions and input are neither valued nor wanted. Abortion access is a vital, necessary part of reproductive healthcare.
“In assessing the health of the nation, the Democrats fetishize ‘the economy’ without specifying who benefits from it. Marcia Fudge, the secretary of Housing and Urban Development, recently bragged on Twitter that 'the United States is the only major economy in the world where the economy as a whole is stronger now than before the pandemic’.
"But whose economy?
"Google has provided its highest paid employees, who were already working remotely, with a $1,000 device so they can also perform rapid Covid tests at home. Meanwhile, shift workers must spend hours waiting to be tested for the virus they are much more likely to have been exposed to.
"As the ruling class has worked safely from home, having goods delivered by human shields, their wealth has increased because they are extracting value from the viral underclass, who are paying with their time on lines, their pathogenic work, and, sometimes, their very lives.”
A damning new report shows that one of the leading COVID-19 vaccine makers appears to have played a role in restricting access to those very vaccines. The report, “Pfizer’s Power,” published this week by the consumer advocacy group Public Citizen, examines Pfizer’s contracts with the United States, United Kingdom, European Commission, Albania, Brazil, Colombia, Chile, Dominican Republic and Peru. They offer a rare glimpse into the power Pfizer has to silence governments, throttle supply, shift risk and maximize profits in the middle of a public health crisis.
#throwbackthursdays Incredible carbon dust illustrations from Leon Schlossberg. Leon had a long and distinguished career at Johns Hopkins, training under the father of modern medical illustration himself, Max Brödel. Artwork courtesy of @yosef_skampson , University of Georgia School of Veterinary Medicine #traditionalartwork #medicalillustrator #residentlife #nurselife #nursesofinstagram #medicalstudent #medstudentlife #proudnurse #medicos #medicosmeme #nursememe #healthcare #hospitallife @medlife_worldwide @ctisus_radiology @sciencestories_ @viral_medical @neurointensivismoblog @doctormedicine_ (at University of Georgia Veterinary Teaching Hospital) https://www.instagram.com/p/CRokNz-FEKY/?utm_medium=tumblr
Cognitive impairment as a result of severe COVID-19 is similar to that sustained between 50 and 70 years of age and is the equivalent to losing 10 IQ points, say a team of scientists from the University of Cambridge and Imperial College London.
The findings, published in the journal eClinicalMedicine, emerge from the NIHR COVID-19 BioResource. The results of the study suggest the effects are still detectable more than six months after the acute illness, and that any recovery is at best gradual.
There is growing evidence that COVID-19 can cause lasting cognitive and mental health problems, with recovered patients reporting symptoms including fatigue, ‘brain fog’, problems recalling words, sleep disturbances, anxiety and even post-traumatic stress disorder (PTSD) months after infection. In the UK, a study found that around one in seven individuals surveyed reported having symptoms that included cognitive difficulties 12 weeks after a positive COVID-19 test.
To explore this link in greater detail, researchers analysed data from 46 individuals who received in-hospital care, on the ward or intensive care unit, for COVID-19 at Addenbrooke’s Hospital, part of Cambridge University Hospitals NHS Foundation Trust. 16 patients were put on mechanical ventilation during their stay in hospital. All the patients were admitted between March and July 2020 and were recruited to the NIHR COVID-19 BioResource.
The individuals underwent detailed computerised cognitive tests an average of six months after their acute illness using the Cognitron platform, which measures different aspects of mental faculties such as memory, attention and reasoning. Scales measuring anxiety, depression and post-traumatic stress disorder were also assessed. Their data were compared against matched controls.
This is the first time that such rigorous assessment and comparison has been carried out in relation to the after effects of severe COVID-19.
COVID-19 survivors were less accurate and with slower response times than the matched control population – and these deficits were still detectable when the patients were following up six months later. The effects were strongest for those who required mechanical ventilation. By comparing the patients to 66,008 members of the general public, the researchers estimate that the magnitude of cognitive loss is similar on average to that sustained with 20 years ageing, between 50 and 70 years of age, and that this is equivalent to losing 10 IQ points.
Survivors scored particularly poorly on tasks such as verbal analogical reasoning, a finding that supports the commonly-reported problem of difficulty finding words. They also showed slower processing speeds, which aligns with previous observations post COVID-19 of decreased brain glucose consumption within the frontoparietal network of the brain, responsible for attention, complex problem-solving and working memory, among other functions.
Professor David Menon from the Division of Anaesthesia at the University of Cambridge, the study’s senior author, said: “Cognitive impairment is common to a wide range of neurological disorders, including dementia, and even routine ageing, but the patterns we saw – the cognitive ‘fingerprint’ of COVID-19 – was distinct from all of these.”
While it is now well established that people who have recovered from severe COVID-19 illness can have a broad spectrum of symptoms of poor mental health – depression, anxiety, post-traumatic stress, low motivation, fatigue, low mood, and disturbed sleep – the team found that acute illness severity was better at predicting the cognitive deficits.
The patients’ scores and reaction times began to improve over time, but the researchers say that any recovery in cognitive faculties was at best gradual and likely to be influenced by a number of factors including illness severity and its neurological or psychological impacts.
Professor Menon added: “We followed some patients up as late as ten months after their acute infection, so were able to see a very slow improvement. While this was not statistically significant, it is at least heading in the right direction, but it is very possible that some of these individuals will never fully recover.”
There are several factors that could cause the cognitive deficits, say the researchers. Direct viral infection is possible, but unlikely to be a major cause; instead, it is more likely that a combination of factors contribute, including inadequate oxygen or blood supply to the brain, blockage of large or small blood vessels due to clotting, and microscopic bleeds. However, emerging evidence suggests that the most important mechanism may be damage caused by the body’s own inflammatory response and immune system.
While this study looked at hospitalised cases, the team say that even those patients not sick enough to be admitted may also have tell-tale signs of mild impairment.
Professor Adam Hampshire from the Department of Brain Sciences at Imperial College London, the study’s first author, said: “Around 40,000 people have been through intensive care with COVID-19 in England alone and many more will have been very sick, but not admitted to hospital. This means there is a large number of people out there still experiencing problems with cognition many months later. We urgently need to look at what can be done to help these people.”
Cognitive impairment as a result of severe COVID-19 is similar to that sustained between 50 and 70 years of age and is the equivalent to losing 10 IQ points, say a team of scientists from the University of Cambridge and Imperial College London.
The findings, published in the journal eClinicalMedicine, emerge from the NIHR COVID-19 BioResource. The results of the study suggest the effects are still detectable more than six months after the acute illness, and that any recovery is at best gradual.
There is growing evidence that COVID-19 can cause lasting cognitive and mental health problems, with recovered patients reporting symptoms including fatigue, ‘brain fog’, problems recalling words, sleep disturbances, anxiety and even post-traumatic stress disorder (PTSD) months after infection. In the UK, a study found that around one in seven individuals surveyed reported having symptoms that included cognitive difficulties 12 weeks after a positive COVID-19 test.
To explore this link in greater detail, researchers analysed data from 46 individuals who received in-hospital care, on the ward or intensive care unit, for COVID-19 at Addenbrooke’s Hospital, part of Cambridge University Hospitals NHS Foundation Trust. 16 patients were put on mechanical ventilation during their stay in hospital. All the patients were admitted between March and July 2020 and were recruited to the NIHR COVID-19 BioResource.
The individuals underwent detailed computerised cognitive tests an average of six months after their acute illness using the Cognitron platform, which measures different aspects of mental faculties such as memory, attention and reasoning. Scales measuring anxiety, depression and post-traumatic stress disorder were also assessed. Their data were compared against matched controls.
This is the first time that such rigorous assessment and comparison has been carried out in relation to the after effects of severe COVID-19.
COVID-19 survivors were less accurate and with slower response times than the matched control population – and these deficits were still detectable when the patients were following up six months later. The effects were strongest for those who required mechanical ventilation. By comparing the patients to 66,008 members of the general public, the researchers estimate that the magnitude of cognitive loss is similar on average to that sustained with 20 years ageing, between 50 and 70 years of age, and that this is equivalent to losing 10 IQ points.
Survivors scored particularly poorly on tasks such as verbal analogical reasoning, a finding that supports the commonly-reported problem of difficulty finding words. They also showed slower processing speeds, which aligns with previous observations post COVID-19 of decreased brain glucose consumption within the frontoparietal network of the brain, responsible for attention, complex problem-solving and working memory, among other functions.
Professor David Menon from the Division of Anaesthesia at the University of Cambridge, the study’s senior author, said: “Cognitive impairment is common to a wide range of neurological disorders, including dementia, and even routine ageing, but the patterns we saw – the cognitive ‘fingerprint’ of COVID-19 – was distinct from all of these.”
While it is now well established that people who have recovered from severe COVID-19 illness can have a broad spectrum of symptoms of poor mental health – depression, anxiety, post-traumatic stress, low motivation, fatigue, low mood, and disturbed sleep – the team found that acute illness severity was better at predicting the cognitive deficits.
The patients’ scores and reaction times began to improve over time, but the researchers say that any recovery in cognitive faculties was at best gradual and likely to be influenced by a number of factors including illness severity and its neurological or psychological impacts.
Professor Menon added: “We followed some patients up as late as ten months after their acute infection, so were able to see a very slow improvement. While this was not statistically significant, it is at least heading in the right direction, but it is very possible that some of these individuals will never fully recover.”
There are several factors that could cause the cognitive deficits, say the researchers. Direct viral infection is possible, but unlikely to be a major cause; instead, it is more likely that a combination of factors contribute, including inadequate oxygen or blood supply to the brain, blockage of large or small blood vessels due to clotting, and microscopic bleeds. However, emerging evidence suggests that the most important mechanism may be damage caused by the body’s own inflammatory response and immune system.
While this study looked at hospitalised cases, the team say that even those patients not sick enough to be admitted may also have tell-tale signs of mild impairment.
Professor Adam Hampshire from the Department of Brain Sciences at Imperial College London, the study’s first author, said: “Around 40,000 people have been through intensive care with COVID-19 in England alone and many more will have been very sick, but not admitted to hospital. This means there is a large number of people out there still experiencing problems with cognition many months later. We urgently need to look at what can be done to help these people.”
On the same day in March 2020 that President Donald Trump declared the COVID-19 pandemic a national emergency, researchers at the Larry A. Green Center in Virginia launched an ongoing survey of COVID-19’s effects on primary care practices. Over the past 2 years, more than 36 000 survey responses from clinicians across the country have painted an alarming picture of a workforce that’s increasingly burned out, traumatized, anxious, and depressed. As Green Center codirector Rebecca S. Etz, PhD, summed up her survey’s findings in a recent interview with JAMA, “It’s been bad for primary care over the pandemic and it’s getting worse.”
Another national health care worker survey, the Coping With COVID study, found that burnout approached 50% in 2020 among 9266 physicians across medical disciplines. Last year’s survey results, which haven’t been published yet, are more dire still, according to study coauthor Mark Linzer, MD, a professor of medicine at the University of Minnesota whose research focuses on burnout. His takeaway: burnout has increased considerably as the pandemic has dragged on.
“It has been a very, very trying 2 years for the clinician workforce, and the health care workforce in general,” Linzer said in an interview. “Particularly over the last 6 months, I think people have really just needed to process what they’ve been through and have time to recuperate. But there really has not been time, given all the pent-up demand for care and the continuing pandemic and the Omicron surge.”
Meanwhile, Lotte Dyrbye, MD, MHPE, chief well-being officer for the University of Colorado School of Medicine, said that some physicians have had the opposite experience during the pandemic—too little work. “An important thing to realize is that how the pandemic has affected physicians is incredibly heterogeneous,” she said in an interview.
Many medical specialties saw the workload decrease in the pandemic’s first year and even during subsequent surges, when demand for non–COVID-19–related visits and elective procedures evaporated. Some practices watched their business and finances dry up. Experts warn that the COVID-19 pandemic, now entering its third year, has pushed an already fragile workforce to the brink. For many clinicians the workplace challenges—ranging from high stress and burnout to understaffing and reduced income, often in combination—have become insurmountable.
Staffing Struggles
Worsening staffing issues are now the biggest stressor for clinicians. Health care worker shortages, especially in rural and otherwise underserved areas of the country, have reached critical and unsustainable levels, according to the National Institute for Occupational Safety and Health (NIOSH).
“The evidence shows that health workers have been leaving the workforce at an alarming rate over the past 2 years,” Thomas R. Cunningham, PhD, a senior behavioral scientist at NIOSH, wrote in a statement emailed to JAMA.
In the absence of national data, Etz says the Green Center data point to a meaningful reduction in the primary care workforce during the pandemic. In the February 2022 survey, 62% of 847 clinicians had personal knowledge of other primary care clinicians who retired early or quit during the pandemic and 29% knew of practices that had closed up shop. That’s on top of a preexisting shortage of general and family medicine physicians. “I think we have a platform that is collapsed, and we haven’t recognized it yet,” Etz said.
In fact, surveys indicate that a “great clinician resignation” lies ahead. A quarter of clinicians said they planned to leave primary care within 3 years in Etz’s February survey. The Coping With COVID study predicts a more widespread clinician exodus: in the pandemic’s first year, 23.8% of the more than 9000 physicians from various disciplines in the study and 40% of 2301 nurses planned to exit their practice in the next 2 years. (The Coping With COVID study was funded by the American Medical Association, the publisher of JAMA.)
A lesson that’s been underscored during the pandemic is that physician wellness has a lot to do with other health workers’ satisfaction. “The ‘great resignation’ is affecting a lot of our staff, who don’t feel necessarily cared for by their organizations,” Linzer said. “The staff are leaving, which leaves the physicians to do more nonphysician work. So really, in order to solve this, we need to pay attention to all of our health care workers.”
Nurses who said they intended to leave their positions within 6 months cited 3 main drivers in an American Nurses Foundation survey: work negatively affecting their health and well-being, insufficient staffing, and a lack of employer support during the pandemic.
“Health care is a team sport,” L. Casey Chosewood, MD, MPH, director of the NIOSH Office for Total Worker Health, wrote in the agency’s emailed statement. “When nurses and other support personnel are under tremendous strain or not able to perform at optimal levels, or when staffing is inadequate, the impact flows both upstream to physicians who then face a heavier workload and loss of efficiency, and downstream impacting patient care and treatment outcomes.”
The Pandemic in Primary Care
The pandemic began to take its toll on primary care clinicians early on, says Etz, who is a professor in the department of family medicine and population health at Virginia Commonwealth University. Although primary care offices typically handle the vast majority of respiratory infections in the community, they weren’t prioritized for personal protective equipment (PPE) and other crucial supplies when COVID-19 struck. “Our survey showed, going as far as 6 months into the pandemic, half the [clinicians] still didn’t have PPE,” Etz said. “People were wearing coffee filters and garbage bags to take care of their patients.”
The Green Center survey showed that primary care clinicians’ stress levels improved last summer as vaccines became widely available in the US, but the Delta variant surge reversed this. Since then, physician mental and physical exhaustion has returned to prevaccine levels.
As of this February, only about a fifth of Green Center survey respondents were fully staffed, and 44% had open clinician positions they could not fill. Still, 40% of respondents said they had taken on an influx of new patients whose previous practices closed. The pandemic also required primary care practices to provide new or expanded services—telehealth, home monitoring of patients with COVID-19, and more mental health care, to name a few.
They’ve done all this with limited resources. Throughout the public health crisis, primary care physician practices have struggled with low reimbursement for telehealth and long-overdue payments from insurers, Etz says. Applying for aid, such as Paycheck Protection Program (PPP) or Small Business Association (SBA) loans, was onerous and itself often costly. “The primary care practices that I know that were able to get money from PPP and the SBA loans that were available had to hire accountants to help them figure out how to do it,” Etz said. Unpublished data from various states and task forces suggest that less than 5% of health care sector financial assistance may have gone to primary care, she noted.Trying to do more for patients while dealing with shrinking staff and resources—all during an unprecedented infectious disease crisis—has left some clinicians traumatized. “In our qualitative comments,” Etz said of the Green Survey, “we still get people sharing suicidal ideation. Talking about panic attacks in their sleep and pulling over on their way to work to puke because they’re under so much stress.” Recent survey responses reflect the ongoing distress:
“I cannot continue to work at this pace and retire at 65. I am 50. I am chronically exhausted. There is no relief in sight.”
“I’m burned out. The patients have so much anxiety and it has affected me. I see 21 patients daily for relatively low pay. I’m on my way out of this position—I can’t remain healthy and stay here.”
“I am emotionally traumatized and experiencing severe burnout. I would quit if I was able.”
“I had planned to work for at least 10 more years, now I’m thinking about ways to retire as soon as possible.”
“I have been in practice for over 30 years and have never felt so emotionally and physically drained as I have this year. I have given up trying to correct COVID misinformation and this is so very discouraging.”
“I’ve exited practice. Pray I don’t ever need to go back. It’s miserable with no positive indicators for improvement.”
More Than Words
Etz, who trained as a cultural anthropologist, sees a troubling pattern in the responses: lack of hope. Hopelessness was also apparent in a mid-2021 survey by the nonprofit Physicians Foundation. About 20% of 2504 physicians said they knew a physician who had either considered, attempted, or died by suicide during the COVID-19 pandemic.
Today, frontline clinicians are experiencing high rates of depression, anxiety, sleep disturbance, and posttraumatic stress disorder, according to Dyrbye, who is a member of the National Academies of Medicine’s Clinician Well-being Collaborative. “Many of them are running on the very last steam,” she said. She noted that compassion fatigue, a result of high levels of work stress, has also set in for some: “They’re getting tired of taking care of patients who are incredibly sick and aren’t vaccinated.”
“There’s clearly still widespread burnout, fatigue, and frustration not only related to the earlier phases of the pandemic, but also the aftermath related to shortage of staffing,” Lou Baptista, MD, MPH, executive vice chair of the department of psychiatry at Columbia University Medical Center (CUMC), said in an interview.
As a result, some physicians are cutting their clinical hours for the first time or jumping ship to different institutions where they feel they’ll be better cared for. Baptista says that many mental health professionals at CUMC are leaving for private practice, where they can work fewer days, make more money, and practice telemedicine from the comfort of their own home.
An important mitigator of health care burnout and intention to leave, it turns out, is feeling valued by one’s organization, which Linzer says requires more from employers than simply expressing the sentiment. Dyrbye says health care organizations must undertake systemic steps to improve the work environment. That means finding ways to reduce workload, improve work efficiency, maximize teamwork, and promote a culture of wellness.
Modeling Change
Early in the pandemic, when time off wasn’t a reality for New York City’s frontline health workers, Baptista helped organize a group of CUMC psychologists and psychiatrists who began volunteering their services to other clinicians in the health system. The program, called CopeColumbia, offered 30-minute peer-to-peer telehealth support sessions, small group sessions customized for different clinical departments, and larger webinars and town halls devoted to topics like stress, trauma, and grief.
“Our thinking was, can we create these brief spaces of just half an hour to give them support,” said Baptista, who last year was named chief well-being officer at ColumbiaDoctors. About a third of the early peer-to-peer sessions led to referrals for clinical care. Over the past 24 months, CopeColumbia has expanded to become the main platform that provides well-being resources and peer support to all medical center employees, not just clinicians.
Last year, NIOSH launched a campaign to address health worker stress, burnout, depression, anxiety, substance use disorders, and suicidal behavior—long-standing problems exacerbated by the pandemic. A goal of the Health Worker Mental Health Initiative is system-wide, organizational-level improvements. The program’s research, funded by the American Rescue Plan Act, could help inform fundamental changes to health care worker shifts, workloads, benefits, time off, and more.
NIOSH’s Chosewood acknowledged the challenge ahead: “The design of work in healthcare needs an overhaul,” he wrote. “Ideally, health worker jobs are so well-designed that doctors, nurses and technicians go home at the end of a fulfilling work day even healthier than when they arrived. I don’t think that’s a pipe dream.”
Linzer agrees that changes are overdue to reduce burnout. “I think there’s a lot of ways that things could be done differently—a lot of work that could be done by others, that would give a chance for physicians to grieve, debrief, heal, and then continue again,” he said. “But the idea of just rushing to start again is, I think, not going to work.”
I’ve always felt really lucky with my doctor, but today really drove home just how much I lucked out with him, especially after some of the absolute horror stories I’ve seen.
I’m fat. Very fat, some would say. My doctor has never made me feel ashamed of that. He’s never dismissed symptoms I’ve had for my health issues by trying to get me to lose weight. And I’ve had plenty of doctors who do that.
Today I had a follow up for some blood work because I have an enlarged thyroid. My cholesterol is a bit elevated since my last test, but still in the ‘normal’ range. Not high enough to need medication, but still enough that we discussed some ways to lower it. He’s focused on diet because I’m physically disabled which rules out most exercise. He’s also ordering more tests to make sure that it isn’t being caused by a liver problem or anything like that.
Then he went on an angry rant about how fatphobic medicine is irresponsible and dangerous, and how a lot of patients who are overweight and have health issues are overweight because of the health problems, not the other way around. So patients like me with limited mobility, or people with pcos causing weight gain and that sort of thing.
I almost left the office crying because I’m so used to specialists being like ‘Oh yeah, your joints don’t work because you’re fat.’ as if I walk on my fingertips like a fucking horse, that even though he’s never been weight focused in my healthcare, I still wasn’t expecting him to be as supportive as he was.
The week provides the opportunity for participants to promote overall awareness for the wide ranging aspects of wellbeing, including social, physical, emotional, financial, career and environmental.
This week, 22-26 June, 2020 is World Wellbeing Week. The observance began in Jersey, the Channel Islands in 2019 and has since been taken up across the world.
Wellbeing and healthy lifestyle concept
Since the beginning of the global lockdown, people have been encouraged to maintain some sort of physical activity or exercise. While it is known that exercise is beneficial for overall physical and mental health and wellbeing, researchers from the University of Cambridge and University of Edinburgh UK, have released a study in which they say that physical activity prevents 3.9 million early deaths each year.
Publishing their work in The Lancet Global Health the researchers said that there is often too much focus on the negative health consequences of poor levels of physical activity, when we should be celebrating what we gain from physical activity.
Exercises and warm up before run
Researchers from the Medical Research Council Epidemiology Unit at the University of Cambridge looked at previously published data for 168 countries which covered the proportion of the population meeting WHO global recommendation of at least 150 minutes of moderate-intensity throughout the week or 75 minutes of vigorous-intensity activity.
By combining these data, with estimates of the relative risk of dying early for active people compared to inactive people, the researchers were able to estimate the proportion of premature deaths that were prevented because people were physically active.
They found that globally, due to physical activity, the number of premature deaths was an average 15% lower than it would have been, equating to 3.9 million lives saved each year. Despite the considerable variation in physical activity levels between countries, the positive contribution of physical activity was remarkably consistent across the globe, with a broad trend towards a greater proportion of premature deaths averted for low and middle income countries.
Hands holding red heart representing healthy heart and wellbeing
The researchers argue that the debate on physical activity has often been framed in terms of the number of early deaths due to the lack of exercise, currently estimated at 3.2 million each year. But showing how many deaths are averted it might be possible to frame the debate in a positive way which could have benefits for policy and population messaging.
Fitness session
Dr Tess Strain from the Medical Research Council Epidemiology Unit at the University of Cambridge said; ‘We’re used to looking at the downsides of not getting enough activity – whether that’s sports or a gym or just a brisk walk after lunch time. But by focusing on the number of lives saved, we can tell a good news story of what is already being achieved…We hope our finding will encourage governments and local authorities to protect and maintain services in these challenging times.’
Written by Muriel Cozier. You can find more of her workhere.
The Lancet Global HealthDOI:10.1016/s2214-109X(20)30211-4
In this round-up we will be looking at some of the developments and challenges surrounding artificial intelligence.
Development and Collaborations
The Organisation for Economic Development (OECD) has launched its Artificial Intelligence (AI) Observatory, which aims to help countries encourage, nurture and monitor the responsible development of trustworthy AI systems for the benefit of society.
The Observatory works with policy communities across and beyond the OECD - from the digital economy and science and technology policy, to employment, health, consumer protection, education and transport policy – considering the opportunities and challenges posed by current and future AI developments in a coherent, holistic manner.
The AI Observatory is being built on evidence-based analysis and provides a centre for the collection and sharing of information on AI, leveraging the OECD’s reputation for measurement methodologies. The Observatory will also engage a wide spectrum of stakeholders from the technical community, the private sector, academia, civil society and other international organisations, providing a hub for dialogue and collaboration.
AI and healthcare
According to a report produced by the European Institute of Innovation and Technology (EIT) Health and The McKinsey Centre for Government (MCG), AI can increase productivity and the efficiency of care delivery, allowing healthcare systems to provide better outcomes for patients.
The WHO estimates that by 2030 the world will be short of 9.9 million doctors, nurses and midwives, which adds to the challenges faced by an already overburdened healthcare system. Supporting the widespread adoption and scaling of AI could help alleviate this shortfall, the report says, by streamlining or even eliminating administrative tasks, which can occupy up to 70% of a healthcare professional’s time.
The issues highlighted, among others, means that ‘AI is now ‘top-of-mind’ for healthcare decision makers, governments, investors and innovators and the EU itself,’ the report states.₁
To fully unlock the potential and capabilities of AI, there is an urgent need to attract and up-skill a generation of data-literate healthcare professionals.
Sustainable Development
Artificial intelligence (AI) is influencing larger trends in global sustainability. Many communities in developing nations do not have access to clean water, which impacts health and has economic and environmental implications.
AI has the capacity and ability to adapt and process large amounts of data in real time. This makes it an ideal tool for managing water resource, whereby utility managers can maximise current revenue, effectively forecasting and planning for the years ahead.
Currently, the development of AI is accelerating, but legal and ethical guidelines are yet to be implemented. In order to prepare the future generations of business leaders and national and international policy makers, the academic community will be playing a large role in this.
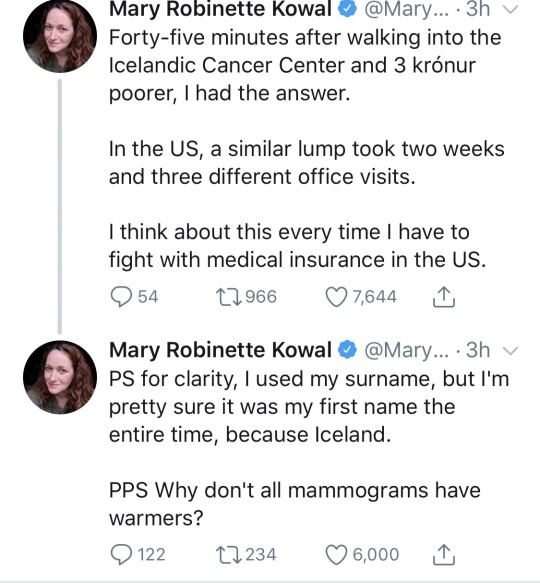
The next time they tell you Americans are “happy” with their employer provided health insurance remember that that “happiness” is fueled by willful ignorance of what the alternatives are really like and fear of losing what little crappy health care they currently have.
Honestly, nevermind the low price, if seeing doctors was this logistically easy I’d have way better health. With adhd/anxiety/depression, seeing doctors is usually just too complicated and takes too much energy to deal with.
I can’t tell you where or how to activate to help solve this. There are politicians, groups, and activists pushing for this in so many ways. I can tell you when, though.
that feeling when you get kicked off of your parent’s insurance for the sin of turning 26 so you have to buy new insurance but literally no insurance provided by your pcp will cover your birth control so you have to pay for it out of pocket, which with your parent’s insurance was only $15 for a three month supply, but now with this new insurance it’s over $800 but you don’t find that out until you get to the pharmacy so naturally you break down crying right here in the CVS with a line of people behind you and you can’t even complain about it because if you even imply that you wish we had free healthcare you get labeled a fucking communist.