Pelagic plastic items are commonly colonized by a diversity of encrusting and fouling animals. Most of these are sessile, hard-shelled or crustose organisms and dominated by moss animals (bryozoans). Also included are barnacles, tube worms, foraminifera, coralline algae, hydroids and bivalve molluscs.
Aggregations of marine debris can provide habitats suiting the larval and juvenile stages of numerous marine organisms. They may also attract free-living, ocean-roaming predators that often gather under fish aggregating devices, and where others simply sought a protective haven.
Example of colonization and encrustation on plastic debris from the New Zealand coastline:
(a) Heavy and varied colonization of a plastic slab recovered (note the hard bodied encrustations and soft fleshy epibionts.
(b) Cuttings from a tangled mass of synthetic rope, carrying a cargo of the warm-water Indo-Pacific oyster, Lopha cristagalli, a species that is alien to New Zealand waters.
(d) Small bryozoan colony (Galeopsis mimicus) attached to a frayed plastic flake (arrowed) recovered from a depth of 393 m off the east coast shelf off the South Island. scale bar 0,2 mm.
During a visual exploration in the north-western Mediterranea using remote operated vehicles (ROVs) a noticeable level of anthropogenic impact was observed in all studied zones,with 158 recorded artificial objects of various types detected.
Different types of anthropogenic impacts observed:
According to scientists consensus, there is no place in the ocean without plastic pollution.
Here are two exaples of excepcional records of acummulation of deep-sea litter in the Japan Trench. Plastic bags in the gap made by a big earthquake off Sanriku in Shinkai, at 6272 m depth (picture a) and the Suruga Bay at 2170 m (in the picture b).
These two records come from a research dive done in 1991 by JAMSTEC.
Ok so Haumea, a dwarf planet beyond Pluto, spins so fast it gets elongated like this. This is just what it looks like. Something deeply unsettles me looking at it. Terrifying.
this is so fucked up
This planet looks like a cool rock someone found in a creek.
one day it’s going to hatch and then all of you will be sorry
I look forward to meeting our dizzy, space hatchling overlord and/or destroyer.
Whole bone marrow cells (BMCs) and bone marrow mononuclear cells (BMMCs) are the most accessible and studied source of stem cells.
BMMCs are isolated from whole bone marrow, and contain a diverse cell population, including mesenchymal stem cells and hematopoietic progenitor cells.
Mesenchymal Stem Cells (MSCs)
MSCs can be isolated from a variety of tissues such as bone marrow, adipose, and umbilical cord; although it is not clear whether their properties are uniform (Selem, Hatzistergos and Hare, 2011).
MSCs are of particular note due to their immunoprivelegednature – a reduced expression of MHC class-I molecule, and lack of MHC class-II and co-stimulatory molecules, means they could potentially be used for allogeneic grafts (Zimmet et al., 2005). This means that they don’t produce an immune response and could be used in transplants - the body won’t reject them.
MSCs inhibit the activity of various immune cells, including T cells, B cells, natural killer cells, and dendritic cells via cell to cell contacts and soluble factors (Laflamme and Murry, 2005).
Foetal and Umbilical Cord Cells
Embryonic stem cells (ESCs), the prototypical stem cell, can develop into all cell types in the body. However, the practical application of human ESCs remains limited due to ethical problems, teratoma formation (cancer), and immune rejection. With rapidly expanding knowledge of molecular and genetic pathways for ESC differentiation, it may become possible to avoid contamination with undifferentiated ESCs, thereby inhibiting teratogenesis when transplanted into the body (Kucia et al., 2006).
Foetal-derived stem cells can also be isolated from the amniotic fluid, which include both pluripotent and committed stem cells.
Umbilical cord cells can be gathered at birth and stored, eg if for treatment later on if a defect is detected in utero.
Induced pluripotent stem cells (iPSCs)
Induced pluripotent stem cells are a more attractive alternative to ESCs, as they are autologous. This means cells can be taken from an individual, ‘reset’ back to their stem cell stage, and then administered to that same individual to avoid rejection. Pluripotency transcription factors are introduced to adult terminally differentiated somatic cells, such as dermal fibroblasts, in a novel strategy which ‘reprograms’ the cells back to an embryonic stem cell-like stage (Yu et al., 2007).
Despite slight epigenetic differences associated with reprogramming, iPSCs fully resemble ESCs in terms of differentiation capacity, morphology and gene expression profile; and have the ability to differentiate into other cells. Ethical and immune response dilemmas are bypassed by the autologous nature of iPSCs, however clinical application is not yet on the horizon due to their teratogenic potential and the oncogenes and virus vectors required for the current method of pluripotent induction (Yamanaka and Takahashi, 2006).
Skeletal myoblasts (SM)
Skeletal myoblasts (satellite cells) are derived from skeletal muscle and have the capacity to differentiate into muscle fibre, which makes them obvious candidates for treating conditions such as heart damage following infarction. However, clinical trials have been halted as SM have been observed to couple with resident cardiomyocytes, resulting in dysfunctional electrocardiology and arrhythmias, and have struggled to transdifferentiate into cardiomyocytes in vivo (Reinecke, Poppa and Murry, 2002).
Stem cells are cells in the body that don’t yet have any role (undifferentiated or partially differentiated), and can change to become almost any cell type.
Canproliferate (divide to make more cells) indefinitelyto make more of the same stem cells.
They are the earliest type of cell in a cell lineage (if a cell was an adult human, stem cells would be the foetus)
found in both embryonic and adult organisms, but they have slightly different properties in each
Can also be made in a lab by reprogramming other cells - resetting them back to stem cell stage.
Inembryonic development (a baby forming in the womb), pluripotent stem cells develop at the blastocyst stage (3-4 days) and differentiate into all the cells of the human body as the foetus develops.
Stem cells do exist in the adult body, however they are not pluripotent - they are unipotent or multipotent - this means they can only differentiate into one or a few cell types respectively.
Adult stem cells
Adult stem cells are found in a few select locations in the body, known as niches, such as:
the brain
bone marrow
blood and blood vessels
skeletal muscles
liver
gonads
They exist to replenish rapidly lost cell types and include hematopoieticstem cells, which replenish blood and immune cells,basal cells, which maintain the skin epithelium, and mesenchymal stem cells, which maintain bone, cartilage, muscle and fat cells. Adult stem cells are a small minorityof cells.
Malignant lesions of the ovaries include primary lesions arising from normal structures within the ovary and secondary lesions from cancers arising elsewhere in the body.
Signs and symptoms
Bloating; abdominal distention or mass
Pressure effects on the bladder and rectum
Constipation, indigestion, reflux
Vaginal bleeding
Shortness of breath, tiredness, weight loss
Diagnosis
Physical findings are uncommon in early stages. Advanced disease may present with ovarian or pelvic mass, ascites, pleural effusion, or abdominal mass or bowel obstruction.
Pathophysiology
Typicallyspreads to the peritoneal surfaces and omentum.
Occurs via local extension, lymphatic invasion, intraperitoneal implantation, hematogenous dissemination, or transdiaphragmatic passage.
Malignant cells can implant anywhere in the peritoneal cavity but are more likely to implant in sites of stasis along the peritoneal fluid circulation.
Epithelial tumours make up 90% of ovarian tumours. Other histologies include:
Sex-cord stromal tumors
Germ cell tumors
Primary peritoneal carcinoma
Metastatic tumors of the ovary
Epithelial ovarian cancer
Arises from epithelium covering the fimbria of the fallopian tubes, or the ovaries, both of which are derived from the coelomic epithelium.
Found primarily as cystic lesions with solid components.
Surface may be smooth or covered in papillary projections.
Cysts contain fluid from yellow to brown and haemorrhagic.
Four main histologic subtypes:
Serous (from fallopian tube)
Endometrioid (endometrium)
Mucinous (cervix)
Clear cell (mesonephros)
Tumours of low malignant potential
Tumours of low malignant potential (LMP) are a variety of much less aggressive epithelial ovarian cancer, with good prognosis.
LMP tumors can cause a range of symptoms similar to epithelial ovarian cancer, including increasing abdominal girth, an abdominal mass, abdominal pain, abnormal uterine bleeding, urinary symptoms, and gastrointestinal symptoms. They may be asymptomatic and found on routine physical examination or ultrasound scan.
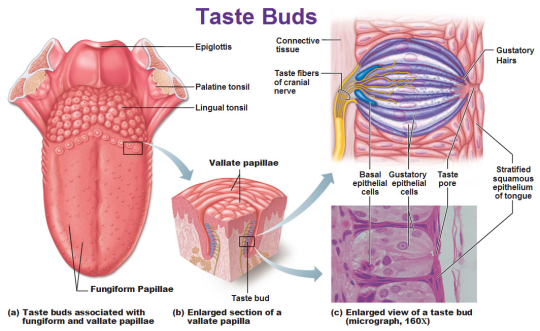
The tongue is covered with many little bumps called papillae.Taste buds are found in the walls of papillae and the grooves surrounding them. Each taste bud contains anywhere from 50 to 150 taste receptor cells.
Microvilliextend from taste receptor cells
and protrude through an opening (taste pore) into the mouth.
These microvilli come in contact with substances in the mouth that can be tasted, also known as tastants.
Tastants interact with taste receptor cells through a number of different mechanisms to depolarize the cells.
When taste cells are depolarized, they release neurotransmitters that stimulate sensory neurons that travel in cranial nerves VII, IX, and X.
These neurons terminate on neurons in the nucleus of the solitary tract in the medulla then continue on to the thalamus.
Taste information is sent to the gustatory cortex, ( ocated on the border between the anterior insula and the frontal operculum).
This information encodes for basic tastes, such as sweet, salty, sour, bitter, and savory or umami.
However, the actual flavour of a food—which is what we typically define as taste—is created by a combination of taste and olfactory (smell) information.
Sweetness
Produced by the presence of sugars, some proteins, and other substances.
Detected by G protein-coupled receptors T1R2+3 (heterodimer) and T1R3 (homodimer).
Saltiness
Saltiness is a taste produced best by the presence of cations (such as Na+, K+or Li+)
Directly detected by cation influx into glial like cells via leak channels causing depolarisation of the cell.
Sourness
Sourness is acidity and is also sensed using ion channels.
Undissociated acid diffuses across the plasma membrane of a presynaptic cell, where it dissociatesin accordance with Le Chatelier’s principle.
Theprotons that are released then block potassium channels, which depolarise the cell and cause calcium influx.
Bitterness
Current research suggests TAS2Rs (taste receptors, type 2, also known as T2Rs) such as TAS2R38 are responsible tasting bitter substances.
Savouriness
The amino acid glutamic acid is responsible for savouriness, but some nucleotides (inosinic acid and guanylic acid) can act as complements.
Glutamic acid binds to a variant of the G protein-coupled receptor, producing a savoury taste
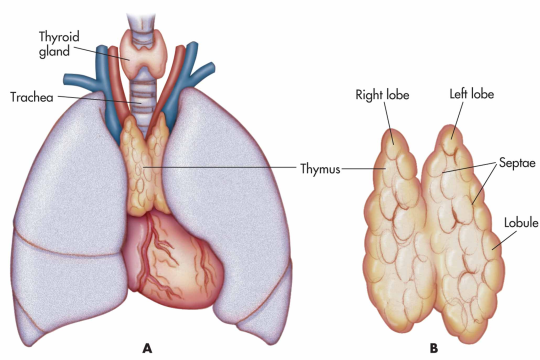
Thethymus is a specialised primary lymphoid organ of the immune system.
At its largest and most active during the neonatal and pre-adolescent periods.
Decreases in size and activity through teenage years
Thymus tissue is gradually replaced by adipose tissue(fat).
Residual T lymphopoiesis continues throughout adult life.
The thymus is composed of two identical lobes and is located in the anterior superior mediastinum, in front of the heart and behind the sternum. Each lobe of the thymus can be divided into a central medulla and a peripheral cortex which is surrounded by an outer capsule.
Function
Facilitates the maturation of T cells - which provide cell-mediated immunity.
T cells begin as hematopoietic precursors from the bone-marrow, and migrate to the thymus, where they are referred to as thymocytes.
In the thymus they undergo a process to ensure the cells react against antigens (“positive selection”), but that they do not react against antigens found on body tissue(“negative selection”).
Once mature, T cells emigrate from the thymus to provide vital functions in the immune system.
Each T cell has a distinct T cell receptor, suited to a specific substance, called an antigen.
Most T cell receptors bind to the major histocompatibility complex on cells of the body.
Positive selection
T cells have distinct T cell receptors. These are formed by process recombination gene rearrangement which is error-prone, and some thymocytes fail to make functional T-cell receptors, whereas other thymocytes make T-cell receptors that are autoreactive. The survival and nature of the T cell then depends on its interaction with surrounding thymic epithelial cells.
T cell receptor interacts with the MHC molecules on the surface of epithelial cells.
A T cell with a receptor that doesn’t react, or reacts weakly will die by apoptosis.
A T cell that does react will survive and proliferate.
A mature T cell expresses only CD4 or CD8, but not both.
Negative selection
T cells that attack the body’s own proteins are eliminated in the thymus. Epithelial cells in the medulla and dendritic cells in the thymus express major proteins from elsewhere in the body. Some CD4 positive T cells exposed to self antigens persist as T regulatory cells.
Pathology
Immunodeficiency - As the thymus is the organ of T-cell development, any congenital defect in thymic genesis or a defect in thymocyte development can lead to a profound T cell deficiency in primary immunodeficiency disease.
Autoimmune disease - Genetic disorders, such as Myasthenia gravis: caused by antibodies that block acetylcholine receptors.
Thymomas - Originate in thymic epithelial cells most often in adults older than 40. Generally detected when they cause symptoms, such as a neck mass or affecting nearby structures such as the superior vena cava. Can be benign; benign but by virtue of expansion, invading beyond the capsule of the thymus (“invasive thyoma”), or malignant (a carcinoma).
Lymphomas - Tumours originating from T cells of the thymus form a subset of acute lymphoblastic leukaemia (ALL)
Thymic cysts - The thymus may contain cysts, usually less than 4 cm in diameter. Thymic cysts are usually detected incidentally and do not generally cause symptoms.
Mathematicians Disprove Conjecture Made to Save Black Holes
Mathematicians have disproved the strong cosmic censorship conjecture. Their work answers one of the most important questions in the study of general relativity and changes the way we think about spacetime.
Nearly 40 years after it was proposed, mathematicians have settled one of the most profound questions in the study of general relativity. In a paper posted online last fall, mathematicians Mihalis DafermosandJonathan Luk have proven that the strong cosmic censorship conjecture, which concerns the strange inner workings of black holes, is false.
“I personally view this work as a tremendous achievement — a qualitative jump in our understanding of general relativity,” emailed Igor Rodnianski, a mathematician at Princeton University.
The strong cosmic censorship conjecture was proposed in 1979 by the influential physicist Roger Penrose. It was meant as a way out of a trap. For decades, Albert Einstein’s theory of general relativity had reigned as the best scientific description of large-scale phenomena in the universe. Yet mathematical advances in the 1960s showed that Einstein’s equations lapsed into troubling inconsistencies when applied to black holes. Penrose believed that if his strong cosmic censorship conjecture were true, this lack of predictability could be disregarded as a mathematical novelty rather than as a sincere statement about the physical world.
“Penrose came up with a conjecture that basically tried to wish this bad behavior away,” said Dafermos, a mathematician at Princeton University.
This new work dashes Penrose’s dream. At the same time, it fulfills his ambition by other means, showing that his intuition about the physics inside black holes was correct, just not for the reason he suspected.
Relativity’s Cardinal Sin
In classical physics, the universe is predictable: If you know the laws that govern a physical system and you know its initial state, you should be able to track its evolution indefinitely far into the future. The dictum holds true whether you’re using Newton’s laws to predict the future position of a billiard ball, Maxwell’s equations to describe an electromagnetic field, or Einstein’s theory of general relativity to predict the evolution of the shape of space-time. “This is the basic principle of all classical physics going back to Newtonian mechanics,” said Demetrios Christodoulou, a mathematician at ETH Zurich and a leading figure in the study of Einstein’s equations. “You can determine evolution from initial data.”
But in the 1960s mathematicians found a physical scenario in which Einstein’s field equations — which form the core of his theory of general relativity — cease to describe a predictable universe. Mathematicians and physicists noticed that something went wrong when they modeled the evolution of space-time inside a rotating black hole.
To understand what went wrong, imagine falling into the black hole yourself. First you cross the event horizon, the point of no return (though to you it looks just like ordinary space). Here Einstein’s equations still work as they should, providing a single, deterministic forecast for how space-time will evolve into the future.
But as you continue to travel into the black hole, eventually you pass another horizon, known as the Cauchy horizon. Here things get screwy. Einstein’s equations start to report that many different configurations of space-time could unfold. They’re all different, yet they all satisfy the equations. The theory cannot tell us which option is true. For a physical theory, it’s a cardinal sin.
“The loss of predictability that we seem to find in general relativity was very disturbing,” said Eric Poisson, a physicist at the University of Guelph in Canada.
Roger Penrose proposed the strong cosmic censorship conjecture to restore predictability to Einstein’s equations. The conjecture says that the Cauchy horizon is a figment of mathematical thought. It might exist in an idealized scenario where the universe contains nothing but a single rotating black hole, but it can’t exist in any real sense.
The reason, Penrose argued, is that the Cauchy horizon is unstable. He said that any passing gravitational waves should collapse the Cauchy horizon into a singularity — a region of infinite density that rips space-time apart. Because the actual universe is rippled with these waves, a Cauchy horizon should never occur in the wild.
As a result, it’s nonsensical to ask what happens to space-time beyond the Cauchy horizon because space-time, as it’s regarded within the theory of general relativity, no longer exists. “This gives one a way out of this philosophical conundrum,” said Dafermos.
This new work shows, however, that the boundary of space-time established at the Cauchy horizon is less singular than Penrose had imagined.
To Save a Black Hole
Dafermos and Luk, a mathematician at Stanford University, proved that the situation at the Cauchy horizon is not quite so simple. Their work is subtle — a refutation of Penrose’s original statement of the strong cosmic censorship conjecture, but not a complete denial of its spirit.
Building on methods established a decade ago by Christodoulou, who was Dafermos’s adviser in graduate school, the pair showed that the Cauchy horizon can indeed form a singularity, but not the kind Penrose anticipated. The singularity in Dafermos and Luk’s work is milder than Penrose’s — they find a weak “light-like” singularity where he had expected a strong “space-like” singularity. This weaker form of singularity exerts a pull on the fabric of space-time but doesn’t sunder it. “Our theorem implies that observers crossing the Cauchy horizon are not torn apart by tidal forces. They may feel a pinch, but they are not torn apart,” said Dafermos in an email.
Because the singularity that forms at the Cauchy horizon is in fact milder than predicted by the strong cosmic censorship conjecture, the theory of general relativity is not immediately excused from considering what happens inside. “It still makes sense to define the Cauchy horizon because one can, if one wishes, continuously extend the space-time beyond it,” said Harvey Reall, a physicist at the University of Cambridge.
Dafermos and Luk prove that space-time extends beyond the Cauchy horizon. They also prove that from the same starting point, it can extend in any number of ways: Past the horizon “there are many such extensions that one could entertain, and there is no good reason to prefer one to the other,” said Dafermos.
Yet — and here’s the subtlety in their work — these nonunique extensions of space-time don’t mean that Einstein’s equations go haywire beyond the horizon.
Remarkable spider with a tail found preserved in amber after 100 million years
An extraordinary new species of arachnid, resembling a spider with a tail, has been discovered in amber from Myanmar (formerly Burma), of mid-Cretaceous age, around 100 million years ago.
The finding is described in a paper appearing Monday in Nature Ecology & Evolution by an international team including Paul Selden of the Paleontological Institute and Department of Geology at the University of Kansas and colleagues from China, Germany, Virginia and the United Kingdom.
“There’s been a lot of amber being produced from northern Myanmar and its interest stepped up about ten years ago when it was discovered this amber was mid-Cretaceous; therefore, all the insects found in it were much older than first thought,” said Selden. “It’s been coming into China where dealers have been selling to research institutions. These specimens became available last year to Nanjing Institute of Geology and Paleontology.”
The new animal resembles a spider in having fangs, male pedipalps, four walking legs and silk-producing spinnerets at its rear. However, it also bears a long flagellum or tail. No living spider has a tail, although some relatives of spiders, the vinegaroons, do have an anal flagellum. Four new specimens have been found, and all are tiny, about 2.5 millimeters body length, excluding the nearly 3-millimeter-long tail.
“Any sort of flagelliform appendage tends to be like an antenna,” the KU researcher said. “It’s for sensing the environment. Animals that have a long whippy tail tend to have it for sensory purposes.”
This exciting new find confirms a prediction made a few years ago by Selden and colleagues when they described a similar tailed arachnid, which resembled a spider but lacked spinnerets. These animals, from the much older Devonian (about 380 million years ago) and Permian (about 290 million years ago) periods, formed the basis of a new arachnid order, the Uraraneida, which lies along the line to modern spiders.
“The ones we recognized previously were different in that they had a tail but don’t have the spinnerets,” said Selden. “That’s why the new one is really interesting, apart from the fact that it’s much younger—it seems to be an intermediate form. In our analysis, it comes out sort of in between the older one that hadn’t developed the spinneret and modern spider that has lost the tail.”
The new animal, called Chimerarachne after the Greek mythological Chimera, a hybrid creature composed of the parts of more than one animal, lies one step closer to modern spiders on account of its possession of spinning organs.
Selden said little of the tiny spider’s day-to-day behavior could be determined.
“We can only speculate that, because it was trapped in amber, we assume it was living on or around tree trunks,” he said. “Amber is fossilized resin, so for a spider to have become trapped, it may well have lived under bark or in the moss at the foot of a tree.”
While the tailed spider was capable of producing silk due to its spinnerets, Selden said it was unlikely to have constructed webs to trap bugs like many modern spiders.
“We don’t know if it wove webs,” said the KU researcher. “Spinnerets are used to produce silk but for a whole host of reasons—to wrap eggs, to make burrows, to make sleeping hammocks or just to leave behind trails. If they live in burrows and leave, they leave a trail so they can find their way back. These all evolved before spiders made it up into the air and made insect traps. Spiders went up into the air when the insects went up into the air. I presume that it didn’t make webs that stretched across bushes. However, like all spiders it would have been a carnivore and would have eaten insects, I imagine.”
Selden said the spider’s remote habitat made it possible that tailed descendants may still be alive in Myanmar’s backcountry to this day.
“We know a lot about the Burmese biota during the Cretaceous,” he said. “It was a pretty good tropical rainforest, and there are a great many other arachnids we know were there, particularly spiders, that are very similar to the ones you find today in the southeast Asian rainforest. It makes us wonder if these may still be alive today. We haven’t found them, but some of these forests aren’t that well-studied, and it’s only a tiny creature.”
Colliding Neutron Stars Could Settle Cosmology’s Biggest Controversy
Newly discovered “standard sirens” provide an independent, clean way to measure how fast the universe is expanding.
To many cosmologists, the best thing about neutron-star mergers is that these events scream into space an otherwise close-kept secret of the universe. Scientists combined the gravitational and electromagnetic signals from the recently detected collision of two of these stars to determine, in a cleaner way than with other approaches, how fast the fabric of the universe is expanding — a much-contested number called the Hubble constant.
In the days since the neutron-star collision was announced, Hubble experts have been surprised to find themselves discussing not whether events like it could settle the controversy, but how soon they might do so.
Scientists have hotly debated the cosmic expansion rate ever since 1929, when the American astronomer Edwin Hubble first established that the universe is expanding — and that it therefore had a beginning. How fast it expands reflects what’s in it (since matter, dark energy and radiation push and pull in different ways) and how old it is, making the value of the Hubble constant crucial for understanding the rest of cosmology.
And yet the two most precise ways of measuring it result in different answers, with a curious 8 percent discrepancy that “is currently the biggest tension in cosmology,” said Dan Scolnic of the University of Chicago’s Kavli Institute for Cosmological Physics. The mismatch could be a clue that cosmologists aren’t taking into account important details that have affected the universe’s evolution. But to see if that’s the case, they need an independent check on the measurements.
Neutron-star collisions — newly detectable by the Laser Interferometer Gravitational-Wave Observatory (LIGO) and Virgo detectors — seem to be just the thing.
“This first [collision] gives us a seat at the cosmology table,” Daniel Holz, an astrophysicist with the University of Chicago and LIGO who was centrally involved in the new Hubble measurement, said in an email. “And as we get more, we can expect to play a major role in the field.”
In an expanding universe, the farther away an astronomical object is, the faster it recedes. The Hubble constant says how much faster. Edwin Hubble himself estimated that galaxies move away from us 500 kilometers per second faster for each additional megaparsec of distance between us and them (a megaparsec is about 3.3 million light-years). This was a gross overestimate; by the 1970s, astrophysicists favored values for the Hubble constant around either 50 or 100 kilometers per second per megaparsec, depending on their methods. As errors were eliminated, these camps met near the middle. However, in the past year and a half, the Hubble trouble has reheated. This time, 67 stands off against 73.
The higher estimate of 73 comes from observing lots of astronomical objects and estimating both distance and velocity for each one. It’s relatively easy to see how fast a star or galaxy is receding by looking at its “redshift” — a reddening in color that happens for the same reason the sound of a receding ambulance’s siren drops in pitch. Correct for an object’s “peculiar velocity,” caused by the gravitational pull of other objects in its neighborhood, and you’re left with its recessional velocity due to cosmic expansion.
Historically, however, it has proven much, much harder to measure the distance to an object — the other data point needed to calculate the Hubble constant.
To gauge how far away things are, astronomers build up rungs on a “cosmic distance ladder” in which each rung calibrates more-distant rungs. They start by deducing the distances to stars in the Milky Way using parallax — the stars’ apparent motion across the sky over the course of the year. With this information, astronomers can deduce the brightness of so-called Cepheid stars, which can be used as so-called “standard candles” because they all shine with a known intrinsic brightness. They then spot these Cepheid stars in nearby galaxies and use them to calculate how far away the galaxies must be. Next, the Cepheids are used to calibrate the distances to Type Ia supernovas — even brighter (though rarer) standard candles that can be seen in faraway galaxies.
The Planck team started from the faint drizzle of ancient light called the cosmic microwave background (CMB), which reveals the universe as it looked at a critical moment 380,000 years after the Big Bang. The CMB snapshot depicts a simple, nearly smooth, plasma-filled young universe. Pressure waves of all different wavelengths rippled through the plasma, squeezing and stretching it and creating subtle density variations on different length scales.
At the moment recorded in the CMB, pressure waves with particular wavelengths would have undergone just the right fraction of an undulation since the Big Bang to all reach zero amplitude, momentarily disappearing and creating smooth plasma densities at their associated length scale. Meanwhile, pressure waves with other wavelengths undulated just the right amount to exactly peak in amplitude at the critical moment, stretching and squeezing the plasma to the full extent possible and creating maximum density variations at their associated scales.
These peaks and troughs in density variations at different scales, which can be picked up by telescopes like Planck and plotted as the “CMB power spectrum,” encode virtually everything about the young universe. The Hubble constant, in particular, can be reconstructed by measuring the distances between the peaks. “It’s a geometric effect,” explained Leo Stein, a theoretical physicist at the California Institute of Technology: The more the universe has expanded, the more the light from the CMB has curved through expanding space-time, and the closer together the peaks ought to appear to us.
Other properties of nature also affect how the peaks end up looking, such as the behavior of the invisible “dark energy” that infuses the fabric of the cosmos. The Planck scientists therefore had to make assumptions about all the other cosmological parameters in order to arrive at their estimate of 67 for the Hubble constant.
The similarity of the two Hubble measurements “is amazing” considering the vastly different approaches used to determine them, said Wendy Freedman, an astrophysicist at the University of Chicago and a pioneer of the cosmic distance ladder approach. And yet their margins of error don’t overlap. “The universe looks like it’s expanding about eight percent faster than you would have expected based on how it looked in its youth and how we expect it to evolve,” Adam Riess of Johns Hopkins University, who led the SH0ES team, told Scientific American last year. “We have to take this pretty darn seriously.”
The 67-versus-73 discrepancy could come down to an unknown error on one side or both. Or it might be real and significant — an indication that the Planck team’s extrapolation from the early universe to the present is missing a cosmic ingredient, one that changed the course of history and led to a faster expansion rate than otherwise expected. If a hypothesized fourth type of neutrino populated the infant universe, for instance, this would have increased the radiation pressure and affected the CMB peak widths. Or dark energy, whose repulsive pressure accelerates the universe’s expansion, might be getting denser over time.
Suddenly, neutron-star collisions have materialized to cast the deciding vote.
The crashing stars serve as “standard sirens,” as Holz and Scott Hughes of the Massachusetts Institute of Technology dubbed them in a 2005 paper, building on the work of Bernard Schutz 20 years earlier. They send rushes of ripples outward through space-time that are not dimmed by gas or dust. Because of this, the gravitational waves transmit a clean record of the strength of the collision, which allows scientists to “directly infer the distance to the source,” Holz explained. “There is no distance ladder, and no poorly understood astronomical calibrations. You listen to how loud the [collision] is, and how the sound changes with time, and you directly infer how far away it is.” Because astronomers can also detect electromagnetic light from neutron-star collisions, they can use redshift to determine how fast the merged stars are receding. Recessional velocity divided by distance gives the Hubble constant.
From the first neutron-star collision alone, Holz and hundreds of coauthors calculated the Hubble constant to be 70 kilometers per second per megaparsec, give or take 10. (The major source of uncertainty is the unknown angular orientation of the merging neutron stars relative to the LIGO detectors, which affects the measured amplitude of the signal.) Holz said, “I think it’s just pure luck that we’re smack in the middle,” between the cosmic-distance-ladder and cosmic-microwave-background Hubble estimates. “We could easily shift to one side or the other.”
The measurement’s accuracy will steadily improve as more standard sirens are heard over the next few years, especially as LIGO continues to ramp up in sensitivity. According to Holz, “With roughly 10 more events like this one, we’ll get to 1 percent [of error],” though he stresses that this is a preliminary and debatable estimate. Riess thinks it will take more like 30 standard sirens to reach that level. It all depends on how lucky LIGO and Virgo got with their first detection. “I do think the method has the potential to be a game changer,” said Freedman. “How fast this will occur [or] what the rate of these objects will be … we don’t yet know.”
Scolnic, who was part of SH0ES, said his team’s tension with Planck’s measurement is so large that “the standard siren approach doesn’t need to get to 1 percent to be interesting.”
As more standard sirens resound, they’ll gradually home in on the Hubble constant once and for all and determine whether or not the expansion rate agrees with expectations based on the young universe. Holz, for one, is exhilarated. “I’ve dedicated the last decade of my life in the hopes of making one plot: a standard siren measurement of the Hubble. I got to make my Hubble plot, and it is beautiful.”
Judged a middle school county science fair today. I got to hand out ribbons to the kiddos who won! It was great :) Remember to always make some time in your busy grad student schedule to give back. That science fair win in 6th or 8th grade could help push that student into pursuing a career in science.
Today is the #gradtaxwalkout. Don’t forget to call your Senator today and tell them you oppose the tuition waiver language contained in the House Tax Cuts and Jobs Act. Urge them to not support a final bill that contains this language!
I think I printed out more than I actually got to read. There are three stacks of papers with scribbles down the margins and sticky notes all over my wall. Down the rabbit hope I go…..pls send coffee.


")