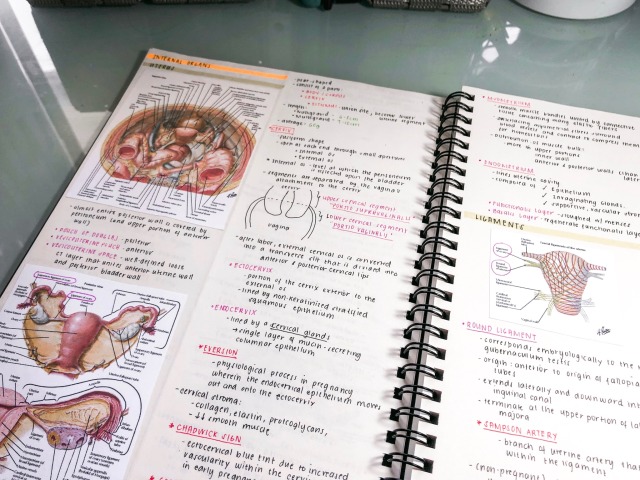
Preparing for my next rotation - Obstetrics and Gynecology! These are my previous notes I made before for pelvic anatomy I miss those days when I had enough time to put a lot of effort into my notes!!!
Because we are total nerds, Testosterone boasts a molecular model beard and Estrogen is sporting the molecular structure for estradiol, one of three types of estrogen made by humans. We especially love the beautiful form of the amino acid chain that comprises Insulin.
“Delicate task wipers” at my gynae appointment today… lol.
Everything looks good by the way, but they’ll call it the repeat Pap comes back abnormal again. If it’s clear, I need another in 6 months and then I’m all set!
Welp, that last post about not anticipating any gyno follow up really bit me in the ass
I was supposed to be having the second of my 6-month follow up Pap smears today. That’s not how it turned out.
My doctor was joking with me that this would be one of the last times I’d be looking at my cervix, and did the smear swab. Then he sprayed with the vinegar solution, and obviously noticed something he didn’t like the look of. He told me he’d be taking a biopsy. While this was a lot better than the first colposcopy I had, it still hurt like a bitch.
Then he said he wanted to do a scraping of the inside of my cervix, in the area he couldn’t see with the colposcope. “Some cramping” ensued, and there was a pretty decent amount of bleeding, so he had to use whatever that peanut butter-looking coagulant stuff is. Unpleasant.
That second scrape made me really nervous because he hasn’t done it before. I’m not sure why he thought it would be needed now, but hopefully he’s just being thorough.
He didn’t book a follow up right away, which makes me feel slightly better, but said he would call with biopsy results in a few weeks.
I asked him about TTC, and he advised me to wait. He said that it would be safer to make sure the biopsy is negative (of course) first, but that if I get pregnant, they can still do some treatment if needed. Usually changes take a long time to develop/worsen, apparently.
So, that’s awesome. Just waiting with baited breath now!
In other news, my last poke/prod of the week is scheduled for Friday when the Humira nurse is coming to my work to do the blood draw for the antibody test.
I got my Mirena four years ago. Right now the Mirena is approved for five years and they are currently working on approving it for more. I chose to get mine replaced a little early because my periods were starting to come back. It’s relatively common for your periods or spotting to start back up on the four or five year mark. Because I have really bad periods and experience gender dysphoria during my periods I wanted to get a new one in ASAP.
If you’d like to read my guide to getting an IUD inserted you can read it here.The procedure for getting it taken out is very similar and many of the same recommendations still apply. I’d definitely still recommend having a buddy, although it isn’t necessarily as bad coming out as it is going in.
At the clinic I went to they didn’t have the Mirena available, only the Liletta and Kyleena. Liletta is approved for 4 years, Kyleena for 5. They are also currently working on approving Liletta for longer so my doctor said that by the time the 4 years are up they’ll probably have it approved for longer. Despite only being recommended for Liletta, and it being a little bigger than Kyleena, is because Liletta has a higher amount of hormones that more closely resemble Mirena. Because I use the IUD to end my periods and I know the Mirena does that I was hoping to get the IUD that most closely matches it.
Below is a detailed recount of my experience. It can get a bit graphic, if you’d like I put the main steps in bold so you can get the gist by just reading that
Once we got the preliminary pregnancy test and consultation over with I was left to take off my pants and get ready for a pelvic exam. It is important for the doctor to take a look and see if they think you may have a vaginal infection before insertion so let them know if you have had any symptoms! This is because if there is an infection while putting in the IUD there is a chance of the infection to spread to the uterus. Turns out I had a yeast infection. Because it had been so hot and muggy apparently a bunch of people had come in with yeast infections so it wasn’t a big surprise. What that meant though was I had to come back a couple weeks after I took antifungals to get rid of the infection.
A couple weeks later I went back and we were finally ready for the insertion. The doctor asked if I was okay having a student come in to observe the process. I said yes because of course I am all about that learning. Know that you should always let your doctor know if you are uncomfortable. My doctor let me know that she likes using the smaller speculums and trying to be as careful as possible. It’s a good idea to tell your doctor if you experience vaginal pain easily, if you’ve experienced any trauma, or if you’re nervous so that they can help you out.
One thing I liked about having a student attend is that the doctor detailed everything going on. That was a fun thing for me, but I know that wouldn’t have been fun for a lot of people. The disadvantage to the student is that the doctor wanted her to try some things on me to learn which meant some things happened twice. The actual taking out and putting the IUD in was handled by the doctor though which was very good.
First the doctor and student checked on my uterus and pelvis by inserting two fingers into the vagina and pressing on various points on my belly/pelvic bone to see if there was any tenderness.
Then the doctor inserted the speculum and located the cervix. On the student’s turn they had trouble finding it which meant they moved the speculum quite a lot and that was not pleasant. Once the doctor helped her find my cervix I breathed again. So far, not much different than a regular pelvic exam.
After they located my cervix they inserted a device to clamp down on the cervix to hold it in place. This is what felt like a pinch. They put on the stuff to numb the cervix and waited a bit before going on. I was told later that the clamping can cause the cervix to bleed a bit, so this can cause some of the irritation you’ll feel later.
Using the strings they were able to pull the IUD out. She showed it to me. I am sad I didn’t think to keep it. You could definitely feel the arms of the “T” come down and then the IUD slide out. It’s not exactly painful, but really weird feeling.If you’re just getting the IUD removed this is as far as you go. They unclamp your cervix and you should probably sit back and relax for a minute before standing up and going about your day.
If you’re getting a new one inserted the next step is to put a sound into the cervix. A sound is a tiny cylandrical object that helps dilate the uterus a tiny bit to help insert it. Sometimes they’ll need to use other methods to help dilate you, but sometimes that is enough. Another reason they use this is that it can go through the cervix into the uterus and it helps them measure the uterus to know where to place the IUD. I found out my uterus is 8 cm, which is perfectly average. Not gonna lie, this part was uncomfortable. The actual going in the uterus wasn’t bad, but once it reached the top of my uterus it kind of hurt and the sensation kind of spread like a wave. What sucked for me is I had to go through it twice, first the doctor did it, then the student. The student apparently didn’t go in far enough so the doctor basically told her to shove it in more and that didn’t feel good. Pretty sure I made a little sound at that point.
When they are able to get an accurate measure of the uterus they use the applicator device to put the IUD in.This is really the most painful part in my opinion, it just feels really weird and like something is definitely trying to move around in your uterus.
After that they cut the strings that hang into the vagina so that they aren’t super long.If you find once you go home the strings are longer than you’d like you can go back and request they trim them a little more. Once you’ve had it for a year or so the strings tend to curl around your cervix out of the way.
This time around I knew what to expect and I stayed laying down.The doctors let me be for a while to let me lay down a bit then with their help sit up. I sat for a while before eventually cleaning up, getting dressed, and sitting back down again. I wore loose pants but where it lay against my belly still hurt. Definitely if you can, wear a dress. Had to hold the seat belt away from my belly while riding home too. Just take it easy and don’t plan to do anything strenuous for a day after. I spotted a bit for a day and I’m still a little sore but it is definitely worth it!
This video introduces the newfound benefits and information that the ultrasound provides, particularly that ultrasounds are non-invasive for both mother and child and relatively inexpensive. Fetal growth and even potential abnormalities can be discovered as they happen in real time. All the ultrasound requires is a full bladder, to provide a water-path for the ultrasound to be viewed.
Just breathe, Angel. Just focus on your breathing, in and out. You’re going to feel some pressure now, but I want you to try and stay as relaxed as possible. Shhhh shh, it’s okay.
Malignant lesions of the ovaries include primary lesions arising from normal structures within the ovary and secondary lesions from cancers arising elsewhere in the body.
Signs and symptoms
Bloating; abdominal distention or mass
Pressure effects on the bladder and rectum
Constipation, indigestion, reflux
Vaginal bleeding
Shortness of breath, tiredness, weight loss
Diagnosis
Physical findings are uncommon in early stages. Advanced disease may present with ovarian or pelvic mass, ascites, pleural effusion, or abdominal mass or bowel obstruction.
Pathophysiology
Typicallyspreads to the peritoneal surfaces and omentum.
Occurs via local extension, lymphatic invasion, intraperitoneal implantation, hematogenous dissemination, or transdiaphragmatic passage.
Malignant cells can implant anywhere in the peritoneal cavity but are more likely to implant in sites of stasis along the peritoneal fluid circulation.
Epithelial tumours make up 90% of ovarian tumours. Other histologies include:
Sex-cord stromal tumors
Germ cell tumors
Primary peritoneal carcinoma
Metastatic tumors of the ovary
Epithelial ovarian cancer
Arises from epithelium covering the fimbria of the fallopian tubes, or the ovaries, both of which are derived from the coelomic epithelium.
Found primarily as cystic lesions with solid components.
Surface may be smooth or covered in papillary projections.
Cysts contain fluid from yellow to brown and haemorrhagic.
Four main histologic subtypes:
Serous (from fallopian tube)
Endometrioid (endometrium)
Mucinous (cervix)
Clear cell (mesonephros)
Tumours of low malignant potential
Tumours of low malignant potential (LMP) are a variety of much less aggressive epithelial ovarian cancer, with good prognosis.
LMP tumors can cause a range of symptoms similar to epithelial ovarian cancer, including increasing abdominal girth, an abdominal mass, abdominal pain, abnormal uterine bleeding, urinary symptoms, and gastrointestinal symptoms. They may be asymptomatic and found on routine physical examination or ultrasound scan.
Hey evryone im felling lonely latelly and wish to find doctor to work on me in open to evry medical stuff from obgyn play to resus and icu play im a good patient please contact me if intrested im open to online had well has irl im in illinois usa and im a 21years old female