#dermatology


⚡Lord Voldermis⚡
A biopsy of a region of skin-that-shall-not-be-named (dermis/hypodermis junction shhh), complete with nerves, vessels, sweat glands and hair follicles.
by @nejiby

A Pacinian Fingerprint at the Scene of the Crime
With all of this criminal activity it’s not surprising the body is full of cells!
A Pacinian or lamellar corpuscle is a mechanoreceptor that is most frequently found at the junction of the dermis/hypodermis in the skin. They are particularly prominent in the skin of the fingers and palms. In addition to the skin they are also found in other organs (e.g. mesentery, pancreas).
These very unique fingerprint-like structures have characteristic whorls formed from concentric lamella. Each lamella is separated from the next by a fluid filled space. And each lamella is lined on its inner and outer surface by connective tissue synthesized by the fibroblasts also in this region (you can see the nuclei of the fibroblasts in these lamellae in this image).
A nerve runs from the inner core of the corpuscle and is responsible for the transduction of mechanical forces applied to the skin into electrical signals that are conveyed to the central nervous system via the dorsal root ganglion.
This organization of fluid filled lamella and a central nerve are highly sensitive to pressure, particularly vibrational forces generated during tasks that involve a manipulative or tactile nature, like sensing the texture of a surface that is touched.
In fact, the screen of the phone/tablet you are using right now has been designed with the specific intention of stimulating the Pacinian corpuscles in your finger as you scroll.
So why not test out the Pacinians of your index finger for a moment by liking this post and following!! :-)
Post link

194 of 366
Just finished my 1 month elective in Dermatology! I can’t put into words to describe how much the world of Derma is amazing. I definitely loved this rotation because I got to see common and rare skin diseases from all over the country! I appreciated the freedom they gave me on letting me do the the whole consultation with patients on my own and let me think of a diagnosis with corresponding management. Of course, they would correct me if needed. I’ve made several mistakes but it was when I learned the most.
I got to stay in their department for a whole month and I feel like I’ve only brushed the surface of their world. There is so much to learn in Dermatology! I now have a newfound appreciation for those who take this honorable path

Ulcerative lesion.
?BCC
#dermatology #surgery #surgeon #medstudent #medschool
https://www.instagram.com/p/CbSvmFkMZ-K/?utm_medium=tumblr
Post link
Can you differentiate by the clinical features?





Can you recall the pathology associated with the condition seen in the pictures?
I’m itchy, constantly. I can’t remember the last time I wasn’t itchy, it’s driving me crazy.
All the dermatologist have to say is, “keep putting your cream on” Well the cream obviously doesn’t work otherwise I wouldn’t of been on toxic drugs for the past 3 years. Putting cream on already irritated skin just makes it worse, even just moisturiser.. But the dermatologists can’t seem to understand that, unless I’m the only one who experiences this.
I’m tired, I don’t want to sleep because when I sleep I scratch, I wake myself up scratching, or my sheets have stook to me from blood and weeping sores so I move then it rips. It just seems never ending.
No one ever thinks that eczema can be this life altering but it is, it affects everything about my life, from not being able to go in then sun due to medications I’m on, what I eat, what I wear.. It’s horrible and nothing seems to be working to get it better. Rant over.
Hey everyone! I’ve not been updating as much lately because there hasn’t been a whole lot that’s new.
Last weekend, I did my second Gutsy Walk for Crohn’s and Colitis Canada! I again made it to Top Pledge Earner status thanks to my generous friends and family, so I guess that’s gonna be my benchmark every year
This week and next, I have three appointments. I saw my family doctor today for a skin check, and he doesn’t like the look of a new mole that popped up on my fourth toe (of all places), so I’m being referred to a dermatologist to likely have it excised. Kinda scary, but I’d also rather be safe about it. So, I guess I’m now adding dermatologist to my collection of doctors, ha ha! (Seriously, I have a GP, GI, rheumatologist, ENT, gynaecological oncologist, endodontist, and I’ve also seen an infectious disease specialist in the past )
Next up is my GI on Thursday, and there’s going to be a lot to discuss. As mentioned, I’m not confident that humira is still as effective as in the past, and I’ve had some odd things going on. The random hive issue, perianal problems, and hair loss that’s returned. I’ve also had major fatigue for the past month, and increased frequency. I’m sure there will be labs ordered, and probably a scope as well. My husband and I are also (we think) FINALLY going to start TTC in the next few months. I want to make sure I have my ducks in a row before we start the process.
Monday next week I have what is hopefully my last repeat pap after my abnormal result and the colposcopy that followed. If it’s all clear, I’m good to go for only having annual paps again! Yay!
So much happening, I’m tired just thinking about it.

I saw the dermatologist today, and had the weird mole on my toe biopsied (which pretty much removed the whole thing).
Back in two weeks to get the stitches out, and the doctor gave me a prescription for Keflex as a precaution to be filled if it gets infected. Obviously toes are already infection-prone, and with an immunosuppressant mixed in, it’s not ideal. He was great about giving me the script in advance, which is not his usual practice. He was very conscious of the effects of Humira, and my history of gross infections, so that was great!
When I go back, he said he should also have biopsy results. He’s pretty confident it wasn’t a melanoma, but if that’s the case, I’ll be referred to a plastic surgeon to have more toe removed ☹️
I’m pretty sure it’s benign but I’m also crossing my fingers! Neither my family doctor, nor the dermatologist really liked the look of it.
Get your skin checks done, Crohnies!
Post link
Researchers identify a bacteria on healthy cats that produces antibiotics against severe skin infections; the findings may lead to new bacteriotherapies for humans and their pets
Researchers at University of California San Diego School of Medicine used bacteria found on healthy cats to successfully treat a skin infection on mice. These bacteria may serve as the basis for new therapeutics against severe skin infections in humans, dogs and cats.
The study, published in eLife on October 19, 2021, was led by Richard L. Gallo, MD, PhD, Distinguished Professor and chair of the Department of Dermatology at UC San Diego School of Medicine, whose team specializes in using bacteria and their products to treat illnesses — an approach known as “bacteriotherapy.”
Skin is colonized by hundreds of bacterial species that play important roles in skin health, immunity and fighting infection. All species need to maintain a diverse balance of healthy skin bacteria to fight potential pathogens.
“Our health absolutely depends on these ‘good’ bacteria,” said Gallo. “They rely on our healthy skin to live, and in return some of them protect us from ‘bad’ bacteria. But if we get sick, ‘bad’ bacteria can take advantage of our weakened defenses and cause infection.”
This is the case with methicillin-resistant Staphylococcus pseudintermedius (MRSP), a bacterium commonly found on domesticated animals that becomes infectious when the animals are sick or injured. MRSP is an emerging pathogen that can jump between species and cause severe atopic dermatitis, or eczema. These infections are common in dogs and cats, and can also occur in humans, though rates of human infection vary around the world. As its name suggests, MRSP is resistant to common antibiotics and has been difficult to treat in clinical and veterinary settings.
To address this, researchers first screened a library of bacteria that normally live on dogs and cats and grew them in the presence of MRSP. From this, they identified a strain of cat bacteria called Staphylococcus felis(S. felis) that was especially good at inhibiting MRSP growth. They found that this special strain of S. felis naturally produces multiple antibiotics that kill MRSP by disrupting its cell wall and increasing the production of toxic free radicals.
“The potency of this species is extreme,” said Gallo. “It is strongly capable of killing pathogens, in part because it attacks them from many sides — a strategy known as ‘polypharmacy.’ This makes it particularly attractive as a therapeutic.”
Bacteria can easily develop resistance to a single antibiotic. To get around this, S. felis has four genes that code for four distinct antimicrobial peptides. Each of these antibiotics is capable of killing MRSP on their own, but by working together, they make it more difficult for the bacteria to fight back.
Having established how S. felis kills the MRSP, the next step was to see whether it could work as a therapy on a live animal. The team exposed mice to the most common form of the pathogen and then added either S. felis bacteria or bacterial extract to the same site. The skin showed a reduction in scaling and redness after either treatment, compared with animals that had no treatment. There were also fewer viable MRSP bacteria left on the skin after treatment with S. felis.
Next steps include plans for a clinical trial to confirm whether S. felis can be used to treat MRSP infections in dogs. Bacteriotherapies like this one can be delivered via topical sprays, creams or gels that contain either live bacteria or purified extract of the antimicrobial peptides.
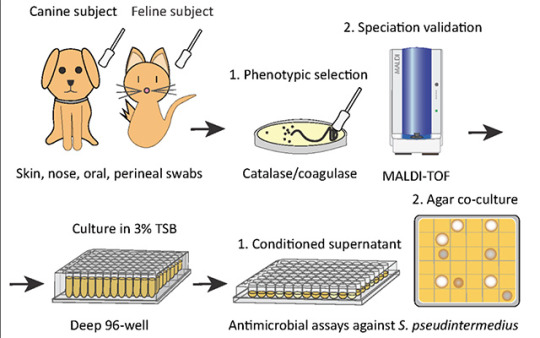
Pictured above: To identify candidates for a new bacteriotherapy against skin infection, researchers first screened various bacteria from dogs and cats and co-cultured them with S. pseudintermedius in liquid and agar antimicrobial assays.
“Cat Bacteria Treats Mouse Skin Infection, May Help You and Your Pets As Well”

I know, it has been a long time since my last post.
Not long after my last update, I stopped taking the medication. It was a decision nourished by many factors.
1. I asked myself why I was taking the medication. Was it for me? Or for others?
2. Weird stomach noises, digestive irregularity.
3. I was training for a marathon, which I completed recently…by the way! I felt that the running was really a lot on my body with the medicine.
Disclaimer: I do not encourage nor do I discourage the usage of Accutane. I remember how I felt when my skin was at its worst. I remember that acne can be more than visually unappealing, but also physically painful (yeah, cysts HURT).
Good news: right now, I’m OKAY with my skin. And that’s a big deal!
Here’s what I’ve been doing, that has personally worked. I can only speak for myself. Different skin requires different treatment. I can say that it has been a while since I have had a painful cyst…and my chin has been clearer than ever and that’s my problem area. Knock on wood that this continues!
1. I don’t wash my face with hot water. I use cold or room temperature. I apply my cleanser (cetaphil daily) and do not rub nor massage my face. I dab the cleanser very lightly. I let it sit on my face for about 10 seconds before rinsing with cold water.
2. After I allow my skin to air dry, I use this aloe vera spray http://www.vitaminlife.com/index/page/product/product_id/76016/product_name/SG+Aloe+Mist?gclid=CjsKDwjw6qnJBRDpoonDwLSeZhIkAIpTR8J2wVikpQ6YVbTNzlpn99G3ilLcNDCJsgUfCZZcgnoeGgKjUfD_BwE
3. After allowing the spray to dry, I apply moisturizer on only my cheeks and forehead. I do not touch or rub it on my chin, since that seems to encourage acne. In the PM, I use the CeraVe tub and in the morning I use the CeraVe moisturizer
This is what I’ve been doing! I’ve also been taking a digestive enzyme to help repair damage that may have been done during my accutane course. I try to eat healthy, but I’m nowhere near perfect. I’m not 100% blemish free, but I’m better than I’ve been a long time…and my face isn’t in pain.
I’d say that’s a victory…
So, right now my face is like 100% clear. Yes. Really. I honestly forgot what that looked like.
And yet, I can’t push away constant ‘2nd thoughts’ about the medication.
So far, I’ve been really lucky. I haven’t had any major side effects. In fact, right now I feel really great. Inside and out. The only thing I have noticed: mild stomach discomfort and persistently strange sounds (from my stomach). Of course this leads to internet searches–and isotretinoin is credited for several digestive and intestinal issues. Then I read more. Things I already knew, but for some reason seem scarier. Like people claiming to have horrible sicknesses and conditions years after their course on the medication.
And sometimes I start asking myself: why did you start taking it? Often, I find my response is pressures from society. Wanting to look good in public, for my partner, etc. etc. Is that an acceptable reason? I don’t know. However, it’s easy to forget the pain of acne (both internal and external) when your face is clear.
I know I never had the most extreme or serious acne. But it was constant, painful, scarring, and I have a serious oil problem.
To stop or to continue.
Does anyone have any thoughts that they would care to share with me? I go back and forth all the time. I’m going to talk to my derm at the end of the week.


I’m so tired. Red eyes and mental fog. Almost every thought is about my skin. How does this lighting make me look? I feel a slight tinge here- will this be a new blemish? Which way should I position my face to show the least amount of acne? Is my current acne product working? When’s my next dermatologist appointment? Will my oily skin ever go away? Are others staring at my skin? What do they see?
I just want a break. I want to be free from these thoughts. To sit, carefree and comfortable, under fluorescent lights.

Dermatology and Dentistry Rotation
This was by far the most relaxed rotation, with only two and a half contact days during the week. Although it was nice to have a bit more spare time than usual, I found it concerning how little time is allocated to the two most common areas of general practice.
On Monday we had a three hour dentistry prac where we practiced nerve blocks and dental extractions on dog cadavers. It was gory, but a really valuable learning exercise. That was it - three hours to become competent dentists!
Wednesday and Thursday were spent in the dermatology clinic, working through real clinical cases, assisting with procedures and practicing diagnostics. The veterinary dermatologist has a bit of a reputation for embarrassing students, which was confirmed within the first half hour when she asked me for the dose rate of Prednisolone in front of the clients. “Errrrr… I don’t remember” was the best I could come up with. She justified the attack by saying I’ll never forget it now, and she’s probably right. For any vet students reading, it’s 0.5-1 mg/kg - stash that one away!
I found dermatology surprisingly interesting, but it was evident that being a veterinary dermatologist would become repetitive pretty quickly. Of the three dog consultations I was involved in, all three had suspected allergies. After hearing the vet’s food trial spiel three times, I feel pretty confident managing an allergy case myself.
On each of our patients, we practiced performing diagnostics such as otoscopic exams, sticky tape preps, superficial and deep skin scrapes, and ear cytology. I witnessed a couple of intradermal allergy tests, which I found really interesting having been through the same process myself for my cat allergy. I also saw an ear flush on a dog, and a skin biopsy procedure on a cat with severe dermatophytosis (ringworm) that had caused deep ulcerative lesions all over the body.
On Thursday afternoon, a couple of the medicine interns taught us how to do skin biopsies on pig trotters. Unfortunately, someone had taken the trotters out of the freezer prematurely and they were well into the decomposition process. The smell had us all retching and gagging, so we worked quickly and finished in record time. I don’t think I’ll be eating pork for a few weeks!
Post link