Creatinine is a waste product produced in muscles from the breakdown of a creatine.
Creatine is part of the cycle that produces energy needed to contract muscles.
Both creatine and creatinine are produced at a relatively constant rate.
Almost all creatinine is excreted by the kidneys, so blood levels are a good measure of how well your kidneys are working.
If low:
Low levels are not common and are not usually a cause for concern.
As creatinine levels are related to the amount of muscle the person has, low levels may be a consequence of decreased muscle mass (such as in the elderly) but may also be occasionally found in advanced liver disease.
If high:
Kidneys break down creatinine - if levels are high, they’re not working properly –>
Damage to or swelling of blood vessels in the kidneys (glomerulonephritis) caused by, eg, infection or autoimmune diseases bacterial infection of the kidneys (pyelonephritis)
Death of cells in the kidneys’ small tubes (acute tubular necrosis) caused, for example, by drugs or toxins
Prostate disease, kidney stone, or other causes of urinary tract obstruction.
Reduced blood flow to the kidney due to shock, dehydration, congestive heart failure, atherosclerosis, or complications of diabetes
Creatinine blood levels can also increase temporarily as a result of muscle injury and are generally slightly lower during pregnancy.
Urea
Urea is the final breakdown product of the amino acids found in proteins. Nitrogen in the form of ammonia is produced in the liver when protein is broken down. The nitrogen combines with other chemicals in the liver to form the waste product urea. Healthy kidneys remove more than 90% of the urea the body produces.
If Low:
Low urea levels are not common and are not usually a cause for concern. They can be seen in severe liver disease or malnutrition but are not used to diagnose or monitor these conditions. Low urea levels are also seen in normal pregnancy.
· If high:
High urea levels suggest poor kidney function.
Acute or chronic kidney disease.
However, there are many things besides kidney disease that can affect urea levels such as decreased blood flow to the kidneys as in congestive heart failure, shock, stress, recent heart attack or severe burns; bleeding from the gastrointestinal tract; conditions that cause obstruction of urine flow; or dehydration.
Albumin
Albumin is the most abundant protein in the blood. It keeps fluid from leaking out of blood vessels; nourishes tissues; and transports hormones, vitamins, drugs, enzymes, and ions like calcium throughout the body. Albumin is made in the liver and is extremely sensitive to liver damage.
If low:
Low albumin concentrations in the blood can suggest liver disease. Liver enzyme tests are requested to help determine which type of liver disease.
Diseases in which the kidneys cannot prevent albumin from leaking from the blood into the urine and being lost.
Also seen in severe inflammation or shock.
Conditions in which the body does not properly absorb and digest protein such as Crohn’s disease.
If high:
High albumin concentrations in the blood usually reflect dehydration.
This is a very long list so click keep reading to read the rest!
Phosphate
In the body, phosphorus is combined with oxygen to form a variety of phosphates (PO4). Phosphates are vital for energy production, muscle and nerve function, and bone growth. They also play an important role as a buffer, helping to maintain the body’s acid-base balance.
If low: (hypophosphataemia)
Hypercalcaemia (high levels of calcium), especially when due to high levels of parathyroid hormone (PTH)
Overuse of diuretics (drugs that encourage urination)
Severe burns
Diabetic ketoacidosis after treatment
Hypothyroidism
Hypokalaemia (low levels of potassium)
Chronic antacid use
Rickets and osteomalacia (due to Vitamin D deficiencies)
Alkaline phosphatase is an enzyme found in high levels in bone and liver. Smaller amounts of ALP are found in the placenta and in the intestines. Each of these makes different forms of ALP (isoenzymes).
Hypophosphatasia (Metabolism disorder, in born). Hypothyroidism. Wilsons disease.
If High:
Raised levels of ALP are usually due to a disorder of either the bone or liver.
If other liver function tests are also raised, this usually indicates that the ALP is coming from the liver.
However, if calcium and phosphate measurements are abnormal, this suggests that the ALP might be coming from bone.
In some forms of liver disease, such as hepatitis, ALP is usually much less elevated than AST or ALT.
However, when the bile ducts are blocked (for example by gallstones, scars from previous gallstones or surgery, or by a tumour), ALP and bilirubin may be increased much more than either AST or ALT.
ALP can also be raised in bone diseases such as Paget’s disease (where bones become enlarged and deformed), in certain cancers that spread to bone or in vitamin D deficiency.
Calcium
99% of calcium is found in the bones, and most of the rest circulates in the blood. Roughly half of calcium is referred to as ‘free’ (or 'ionized’) and is active within the body; the remaining half, referred to as 'bound’ calcium, is attached to protein and other compounds and is inactive.
If low: (hypocalcaemia)
The most common cause of low total calcium is low protein levels, especially low albumin. When low protein is the problem, the 'free’ calcium level remains normal.
High levels of glucose most frequently indicate diabetes, in fasting blood glucose test: <7mmol/L is indicative and in oral glucose test ites <11 mmol/L .
Acromegaly
Acute stress (response to trauma, heart attack, and stroke for instance)
Long-term kidney disease
Cushing’s syndrome
Drugs, including: corticosteroids, tricyclic antidepressants, oestrogens (birth control pills and hormone replacement therapy [HRT]), lithium..
Hyperthyroidism
Pancreatic cancer. Pancreatitis
Triglyceride:
Most triglycerides are found in fat (adipose) tissue, but some circulate in the blood to provide fuel for muscles to work.
If low:
Hyperthyroidism. Malnutrition. Certain medications and drugs can deplete fat, leading to low triglycerides.
If high: (e.g. at least 10-15 mmol/L) –> pancreatitis.
Parathyroid hormone:
Part of a ‘feedback loop’ that includes calcium, PTH, vitamin D, and to some extent phosphate and magnesium. PTH is secreted into the bloodstream in response to low blood calcium concentration.
If both PTH and calcium results are normal, and appropriate relative to each other, then it is likely that the body’s calcium regulation system is functioning properly.
Low –> conditions causing hypercalcaemia, or to an abnormality in PTH production causing hypoparathyroidism.
High –> hyperparathyroidism, which is most frequently caused by a benign parathyroid tumour.
Calcium - PTH Relationship
Calcium low and PTH high, then PTH working. Low calcium may be investigated.
Calcium low and PTH normal or low –> hypoparathyroidism.
Calcium high and PTH –> hyperparathyroidism.
Calcium normal and PTH high –> vitamin D deficiency or chronic kidney disease.
Amylase
Released from the pancreas into the digestive tract to help digest starch. It is usually present in the blood in small quantities. When cells in the pancreas are injured or if the pancreatic duct is blocked (by a gallstone or rarely by a tumour) increased amounts of amylase find their way into the bloodstream.
If high:
Pancreatitis which is a severe inflammation (often 5-10 times normal)
Cancer of the pancreas, gallbladder disease, a perforated ulcer, obstruction of the intestinal tract, mumps or ectopic pregnancy.
Increased blood amylase with normal or low urine amylase may indicate decreased kidney function or the presence of macroamylase.
If AST is higher than ALT,amuscle source of these enzymes should be considered. For example, muscle inflammation due to dermatomyositis may cause AST>ALT. Or complete liver necrosis
Alcoholic fatty liver disease: AST > 8 times the ULN; ALT > 5 times the ULN
Nonalcoholic fatty liver disease: AST and ALT > 4 times the ULN
Acute viral hepatitis or toxin-related hepatitis with jaundice: AST and ALT > 25 times the ULN
Ischemic hepatopathy (ischemic hepatitis, shock liver): AST and ALT > 50 times the ULN (in addition the lactate dehydrogenase is often markedly elevated)
Chronic hepatitis C virus infection: Wide variability, typically normal to less than twice the ULN, rarely more than 10 times the ULN
Chronic hepatitis B virus infection: Levels fluctuate; the AST and ALT may be normal, though most patients have mild to moderate elevations (approximately twice the ULN); with exacerbations, levels are more than 10 times the ULN
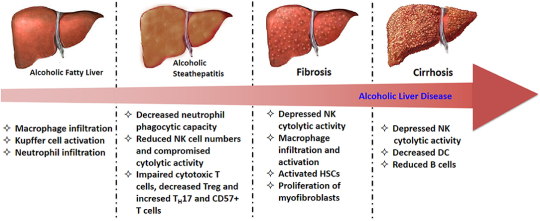
Ethanol is metabolised in the liver toacetaldehydeby alcohol dehydrogenase
which is in turn metabolised to acetate by aldehyde dehydrogenase.
As acetaldehyde is formed, NAD is metabolised to NADH as a cofactor in this reaction.
ThisNADH inhibits the actions of isocitrate dehydrogenase and alpha ketoglutarate and fatty acid oxidation, meaning it favours fatty acid synthesis.
Fat builds up in vacuoles of hepatocytes and mitochondria begin to dysfunction under oxidative stress, creating reactive oxygen species.
This fatty stage is known as steatosis and is stage one of alcoholic liver disease. It is reversible.
Stage Two
Inflammatory cytokines such as IL-6 and TNFa influx in, causing inflammation.
Water begins to accumulate inside hepatocytes and they begin to balloon. This causes significantcholestasis.
The inflammatory cytokines stimulate hepatocytes to produce collagen, which can begin to formfibrosis.
This collagen can be pericellular or around central veins, forming collagen bridges. This is a precursor for cirrhosis.
Stage Three
As the fibrosis progresses,hepatocytes begin to die and cirrhosis occurs.
This is end-stage alcoholic liver disease and can lead to liver failure and death.
Liver function tests
Instage 1; all LFTs will be raised. AST and ALT will be raised by approximately 5-10x the upper reference limit except albumin. They will both usually be below 300IU/L. AST will be raised above ALT; this is different to other hepatic conditions such as cholestasis, tumours, hepatitis, where ALT will be above AST.
In stage 2; ALP and bilirubin will increase significantly as cholestasis occurs and blocks bile duct. This will usually be above 300IU/L, which is different from filtrative diseases, where ALP is usually raised to 200-250IU/L. AST and ALT may increase further.
Instage 3; AST and ALT are between 10-100x the upper reference limit, suggesting significant cirrhosis and damage to cells. AST will remain above ALT. GGT will be raised significantly, which is common with alcoholic liver disease. Albumin will be decreased, suggestive of total liver failure. In other hepatic conditions, liver damage usually does not reach this stage and so albumin stays within the range.
Min Jeong Seo - To live on infusionsbags, roses, 2005
The stalks these flowers are already dried up but their blossoms are preserved and kept fresh by the medical infusin bags. The life-span of every living creature is limited.The infusion bags stand for the progress in medicine and the prolongation of human life.They somehow carry an ambivalent message as they refer to both death and life an the same time. Both states are immanent here. To preserve the beauty of the flowers artifically with the help of the infusion bags points out man’s inclination to repress the fact having to die and to postpone death
Starting clinical rotations can be overwhelming. If you’re like me, you may spend the first days stressing about where you should go, what questions are legit to ask and how you should behave. Most of the time you may have no idea of what your superiors are talking about and you just fake a smile and pretend you know exactly what you’re doing. Meanwhile it’s totally normal to feel lost during the first days of your arrival in a new care unit, it shouldn’t last and you should be able to get more comfortable with the team you’re working with and become more autonomous. Here’s how to get the most of your clinical rotations:
ALWAYS introduce yourself when meeting with a new team : it will always be appreciated and people should be able to reach out to you if they need it
TAKE NOTES and always keep a little notebook in your pocket! I actually own 3 (yes it may be a bit excessive) : one for patient’s history, one for personal notes and another one for definitions and scores
Ask for feedback. The resident you’re shadowing may not necessarily think about giving you a feedback, or maybe he won’t pay enough attention to what you’re doing, and that’s why it’s better if you ask specifically for a feedback, especially when completing a task that you’ve been asked to do.
If there’s a « down » moment when you don’t have anything to do, ask if there’s something you can do for help, even to other members of your team. Don’t hesitate to reach to the nurses or the other medical staff and ask for some teaching! I once spend an entire day with the nurses of my unit so I could learn how to properly draw blood.
If there’s really nothing to do, use this spare time to study a specific subject, and ask your resident if you can present it to him : not only it forces you to study a subject, but you’ll also be able to actively recall it better
Before seeing any patient alone, make sure you went through his medical history so you already know if there’s a specific topic you have to investigate more : be prepared for questions from your assigned residents/physicians!
MAKE THE CALLS. I know, I know, making phone calls is SUPER SCARY (especially when you have to call chiefs and professors). However, I like to say that it’s like running : the more difficult it is, the more you should do it. Prepare what you have to say so you don’t loose yourself during the call, and force yourself to make the phone calls as often as possible. You’ll gain more and more confidence and you won’t be so scared anymore.
NEVER be late.
If you feel there’s something wrong (with you of with a situation) : talk to your assigned resident/physician. They know how overwhelming it can get, so don’t hesitate to reach out for help
Bring snacks. And a big water bottle. Avoid drinking too much coffee.
Being a medical student has many good sides : you can get a first hand-on experience with patients without huge responsibilities, it is the BEST time to make mistakes and ask « silly » questions ! If you don’t do this during this time, you won’t be able to do it later.
Most of the time, you’ll feel like you know nothing, and you’ll forget about things you learned the day before. It’s normal. Don’t be too hard on yourself.
Be patient. And LISTEN.
ENJOY YOUR TIME ! Be curious about everything, make new friends, talk with your patients, see as many things as you can, because this is the only time where you can get all these possibilities!!




download my med school study guid")