Ask Ethan: How Can A Non-Expert Evaluate Conflicting Claims By Actual Experts?
“I assume that you are not an expert on fluoridated drinking water, climate change, or COVID-19 and yet you feel confident that you can identify the correct scientific position on each of these topics. How do you do that and is it something that the average intelligent person can do as well? Isn’t that the real question?”
You’ve been in that awkward situation before: you hear two opinions on an important issue from two different experts. How do you, a non-expert, evaluate which side of an argument is correct?
Seeing friends or extended family by video? You can have a huge impact by talking to them about issues that are important to you. Take the opportunity to discuss health care access for communities of color.
Here are 9 tips for leading the conversation. Remember: Talking with your friends and family about the issues you care about can have a real influence that extends even beyond your circle.
Tip #1: Open the dialogue in a way that’s welcoming.
Share how the last couple of years have affected your views on health and health insurance. Say something like, “I’ve been [concerned/angry] about COVID-19’s disproportionate impact on [Black and Brown communities/our community].”
ASK: “Could we talk about how racist our country’s health care system is? I have some ideas about what can be done, and I’d love to hear your take.”
Tip #2: Get everyone on the same page by defining common terms.
Racism
Racism in America is the outgrowth of white supremacist policies and ideas that assume white people are superior to other racial groups.
Racist policies are written and unwritten laws and customs that cause racial inequity, putting racial groups on unequal footing.
Public Health
Public health is built on the principle of protecting and improving the health of people and their communities.
A public health crisis happens when something threatens the lives and health of an entire community or multiple groups of people.
ASK: Have you [seen/experienced] racism in health care?
Tip #3: Define some terms about race that are less common.
Anti-Blackness refers to a worldwide ideology that devalues being Black.
Anti-Black policies and institutions in white supremacist systems dehumanize and marginalize Black people around the world.
Anti-Black racism covertly disregards and overtly attacks anti-racist policies, Black people, and Black institutions.
Structural racism is a system in which policies, practices, and other norms perpetuate racial inequity. It’s the root cause for the health inequities we see today.
Racial inequity in America blocks Black and Brown people from living freely and safely — while putting white people in power, giving them more resources, and chipping away at their humanity.
Racist health care policies cause health inequities for racial groups, fortifying long-standing barriers and creating new barriers to health care access for Black and Brown communities.
Tip #4: Define some terms about health and fairness that are less common.
Equality vs. Equity
Equality gives everyone the same exact things, but ignores differences. Equal access to COVID-19 testing means everyone could theoretically get a test. But for many people, testing is too expensive and far away, or only open at times where they are unable to take off work or get childcare.
Equity gives everyone what they need, tailored to their individual situation. Equitable access to COVID-19 testing would be affordable, nearby, and have flexible hours for everyone.
Health Inequities vs. Health Equity
Health inequities are systemic, avoidable, and unjust differences in the health of a group of people compared to other groups.
Health disparities are any kind of differences in health outcomes for a group compared to other groups. Disparities don’t refer to social or structural causes like inequities do.
Health equity happens when everyone has a fair and just opportunity to be as healthy as possible. This requires removing obstacles to health such as: poverty, discrimination, powerlessness, limited education, unstable housing, unsafe environments, and lack of health insurance.
Tip #5: Provide examples of racial and health inequities.
Racism is embedded in the structure of the U.S. health care system. The people in charge of that system — including politicians and insurers — have carried out discriminatory practices throughout its history.
Institutionalized discrimination in the U.S. health care system has thrown up roadblocks to insurance, testing, treatment, and care for communities of color. That includes the system’s reliance on employer-sponsored insurance. Because of historic economic barriers, Black and Brown people are less likely to be working in jobs that offer this benefit.
Racial bias among medical researchers and health care providers — such as the erroneous belief that Black people feel less physical pain — have withheld needed care and pain management from Black patients.
Being Black in America takes a toll on the health of Black people.
Racism, microaggressions, and discrimination cause chronic stress.
Researchers have shown that racism stresses and prematurely ages human cells.
All that stress causes physical and psychological harm over time.
The result: increased rates of illness and death among Black people.
Tip #6: Share how health care inequities have led to dramatic disparities in health conditions for Black and Brown communities.
Racial and health inequities help explain why — regardless of income or education — Black and Brown patients have disproportionately fared worse compared to their white counterparts across many health outcomes.
Racism’s chronic stress is linked to higher risk of depression, diabetes, and high blood pressure.
Black people disproportionately experience police-inflicted harassment, violence, injuries, and murder. Living in fear of state-sanctioned brutality causes a host of underlying health problems.
Because of racist policies like redlining, Black and Brown people are more likely to live near toxic sites and amid high pollution, as well as in neighborhoods that lack healthy food options and places to exercise. These environments are linked to higher rates of asthma, respiratory illnesses, and cardiovascular disease.
Long-standing, systemic health and social inequities in the United States and discrimination in doctors’ offices and hospitals all have resulted in a high maternal mortality rate among Black women — three times the rate for white women.
Structural racism, public health failures and economic inequalities — including that the location of Black and Brown workers’ jobs are more likely to put them at risk of catching COVID-19 — have all translated to exponentially higher COVID-19 infection and death rates in Black, Indigenous, and Latino communities.
Tip #7: Discuss why racism is a public health crisis.
The American Medical Association, the American Public Health Association, several states, and other U.S. institutions declared that racism is a public health crisisand called for urgent action from policymakers and institutions.
Discrimination creates barriers to health, both inside and outside the doctor’s office. Your health depends on whether you can access health care, employment, good wages, food security, clean air and water, and stable housing — all of which are hurt by racism.
SCROLL UP: Refer to the definition of “public health crisis” and share how you feel about it.
ASK: “How do you feel about racism being declared a public health crisis?”
Tip #8: Share what federal policies you support to address racial inequity.
For example, you may want them to support policies that:
Aim to eliminate the inequities and biases woven into the fabric of this nation’s institutions, particularly the racial inequities in maternal health.
Provide additional COVID-19 relief that helps Black, Indigenous, and Latino communities — which have been disproportionately ravaged due to ongoing systemic racism and oppressive policies.
Defund the police. Instead of investing in police forces that brutalize Black people, prioritize a public-health approach that strengthens Black communities, promotes community support, and connects people to services.
Support Black organizations and leaders who are at the forefront of the fight to fix the public health crisis that racism presents and the systems that exploit people of color.
Tip #9: Express gratitude for everyone in the conversation.
Thank your friends and family for connecting with you on this issue, and let them know that you’re open to speaking with them again.
Show them some warmth — and give them the time and space to sit with the discussion.
Today is the 20th anniversary of World Asthma Day. The 2018 theme is “Never too early. Never too late. It’s always the right time to address airways disease.” The theme calls attention to the need for diagnoses for patients at all stages of life.
Asthma is the most common chronic disease among children and affects more than a quarter-billion people around the globe, including more than 8% of all children here in the United States.
Those who suffer from asthma also often suffer from allergies. May is National Allergy/Asthma Awareness Month.
There’s already a vaccine that’s 85% effective against monkeypox, hundreds of millions of doses have been stockpiled. 3 years ago I would have found more comfort in that knowledge.
Have you ever stroked a stranger’s hair when they’re sick and told them it’s going to be okay even though you know what the numbers on the screen mean? Holding someone’s hand while they’re crying and telling you they’re scared runs a chill down your spine. Have you ever called someone by a name on a armband but wondered if that’s what their family calls them? Have you ever seen someone close their eyes and wonder if they’ll ever open them again? Have you ever forgotten what color someone’s eyes are? Have you ever been the place holder for their wife, husband, children, mother, or father? Have you ever cried telling that stranger that their family says they love them and that they’re praying for them even when they can’t be there with them? You ever tell that stranger that you’re praying for them too?
Nurses everywhere are tired. Emotionally. Mentally. Physically. We’re all tired.
Very funny that the govt is only giving tests to HOUSEHOLDS and not individuals therein
Correction:
to ADDRESSES
Separate apartments in one building count as separate addresses–look up exactly how your address is recorded by the usps. Some people have also worked around that by putting the apt number in the “street address” box instead of the secondary address line. Usps IS sending them to individual apartments, if yours was blocked you can send a service inquiry to emailus(dot)usps(dot)com/s/the-postal-store-inquiry
A new trial by UC San Diego Health infectious disease specialist Maile Young Karris, MD, will use longitudinal questionnaires and qualitative interviews to assess the impact of living in an interconnected virtual village on the loneliness known to afflict older people with HIV.
“It’s about changing the culture back to how it used to be,” Karris said, “where neighbors actually knew each other and helped each other and you didn’t have to worry so much about your poor dad who lives by himself, far away from you, because you knew that his neighbors would call you if anything happened or would make sure that he was eating.”
Hepatitis A Vaccination Required for Herd Immunity in People Experiencing Homelessness or Who Use Drugs
In the U.S., hepatitis A outbreaks are repeatedly affecting people experiencing homelessness or who use drugs. A 2017-19 Kentucky outbreak primarily among these groups resulted in 501 cases, six deaths. Vaccination efforts likely averted 30 hospitalizations and $490K in costs, but UC San Diego and Oxford researchers say more could have been saved if initiated earlier and faster. They determined herd immunity in these populations requires 77 percent vaccinated, underscoring need for outreach.
The study, published October 18, 2021 in Vaccine, was led by Natasha Martin, DPhil, professor at UC San Diego School of Medicine, and Emmanuelle Dankwa and Christl Donnelly, CBE FMedSci FRS, at University of Oxford.
Pictured: A UC San Diego Health employee is vaccinated against hepatitis A during an outbreak in San Diego, Calif. in 2017. Credit: Erik Jepson/UC San Diego Publications
Free Period: Our OB/GYN Expert Weighs in On New Law for California Schools
Period products will be provided free of charge in public schools across California starting next school year as part of new legislation recently signed into law by Governor Gavin Newsom.
The Menstrual Equity for All Act will require public schools with students in grades six to 12, community colleges and the California State University System to provide the free products in the 2022-2023 academic year.
We asked Alice Sutton, MD, obstetrician/gynecologist at UC San Diego Health, to explain the importance of providing free period products to this population of young women and how a comprehensive approach to women’s health is critical, especially for underserved students.
Question: What are some benefits to having tampons freely available in schools?
Answer: Students experiencing a lack of access to menstrual products, education, hygiene facilities, waste management or a combination of these, may skip school if they don’t have adequate sanitary products, or they may improvise with items, such as paper towels that are not meant for menstrual hygiene.
Period poverty causes physical, mental and emotional challenges. Having menstrual products available in school will help students concentrate on their studies and keep them in class while meeting their health care needs.
Q: Are there concerns about whether there’s enough support in schools to help young women who are menstruating?
A: Young women who are experiencing painful or heavy periods often don’t know that there are safe and effective treatments for these issues. Sometimes the discomfort is bad enough that they miss class or extracurricular activities.
Having a nurse, teacher, coach or other trusted adult in a young women’s life in the school setting provides support and could steer her towards making an appointment with an OB/GYN to discuss options for management, such as lifestyle interventions and medications.
Q: Besides providing tampons, what else should schools be doing to support reproductive health in young people?
A: Appropriate education about the menstrual cycle, tailored to their age-level should be provided. At an even more basic level, some students may not come from homes where they have a parent who they can ask for advice, and so school may be the place where they can find a trusted adult who provides them with accurate information and can point them to appropriate resources.
The American College of Obstetricians and Gynecologists recommends a first reproductive health visit between the ages of 13 and 15. It is a good time to establish care and have a first visit where the adolescent has the opportunity to discuss concerns privately with a doctor. Gynecology visits at this age are tailored to the patient. Topics that might be covered include normal anatomy and normal menstruation, healthy relationships and consent, immunizations, physical activity, substance use including alcohol and tobacco, eating disorders, mental health, sexuality, contraception and pregnancy prevention and sexually transmitted infections.
“This is a groundbreaking study of normal and atypical brain developmental trajectories from day 0 to 10 years of age in a large sample of about 8,000 families,” Christina Chambers, PhD, MPH, professor of pediatrics at UC San Diego School of Medicine and professor in the Herbert Wertheim School of Public Health and Human Longevity Science at UC San Diego.
Policymakers can reduce overdose deaths and other harms stemming from nonmedical use of opioids and other dangerous drugs by switching to a policy of “harm reduction” strategies. Harm reduction has a success record that prohibition cannot match. It involves a range of public health options. These strategies would include medication-assisted treatment, needle-exchange programs, safe injection sites, heroin-assisted treatment, deregulation of naloxone, and the decriminalization of marijuana.
Though critics have dismissed these strategies as surrendering to addiction, jurisdictions that have attempted them have found that harm reduction strategies significantly reduce overdose deaths, the spread of infectious diseases, and even the nonmedical use of dangerous drugs.
Hello! I would like to warn everyone of an experience my roommate and I have just had, in case I can prevent it happening to anyone else. Or, you know, if anyone knows a lawyer who could advise us.
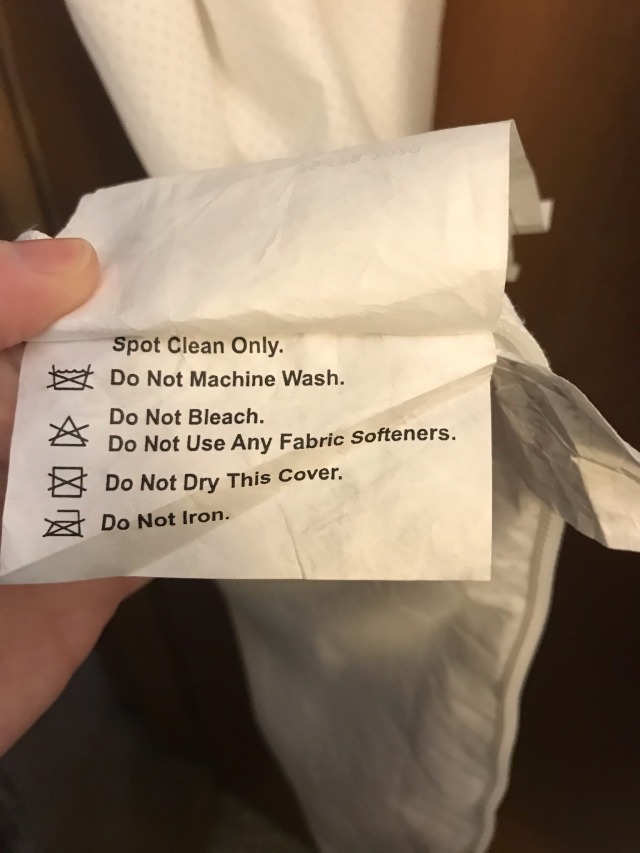
My roommate has a queen size Nectar mattress. Friday night, she spilled some water on the bed and took the cover off to air dry. She unzipped the cover, and a flame retardant sleeve (that we hadn’t known was there to begin with) made of woven fiberglass began shedding small fiberglass particles. They were airborne. The whole room and everything in it is contaminated, and there are few surfaces elsewhere in the apartment that don’t have at least a little. Nowhere on the mattress’ tags or on the Nectar website does it say there is a fiberglass sleeve. In fact, it makes a big deal of how there are five components: top of cover, three layers of foam, bottom of cover. Nothing about the flame retardant sleeve there. The label on the cover doesn’t say you can’t take it off, just that they suggest you don’t. It does not mention fiberglass as a material found in the mattress at all. The website even has a page explaining that you CAN take off the cover and wash it, if you must, just that they suggest you don’t. No real reasons given. No mention of fiberglass.
Our apartment is sparkly with fiberglass. We have had to drop money on a HEPA filter vacuum that could safely remove some of it, and on new non-permeable mattress covers to contain the worst of the source. We have had to garbage-bag up almost everything in her room. No amount of runs through the laundry seems to get it all out of clothes, and we have to thoroughly wipe out the washer and dryer drums every load. All her pillows were ruined, the chair in her room, her clothing, some expensive bras, a nice area rug, and I’m sure there will be trouble on the horizon with our landlord regarding the carpet, even if we do vacuum it as well as we can.
Lilly has been having nosebleeds, before the mattress was unzipped, but the worst one I’ve seen yet was the one that evening. She’s been sleeping on it almost a year, and it could have begun coming through the fabric cover. Nosebleeds are a sign of fiberglass inhalation.
We have contacted the company, and their response was honestly insulting. We were told that we shouldn’t have taken the mattress cover off to begin with, and that it can no longer be covered by the 365 night guarantee, despite us having had it for under the full year. I have just now, after three days trying, finally spoken to someone willing to look into our case, so here’s hoping we’ll get even a fraction of what we are, frankly, owed.
It really feels like there could be some sort of lawsuit here.
In fact, there is one, with a situation nearly identical to ours but with a different company. This was the first hit when I searched our problem online.
Anyway, if you have a Nectar mattress, don’t ever open the easily accessible warning-label-free zipper! If you have had it under a year, and it’s in its original condition, it can still be returned. If you were planning to get one, maybe don’t! A lot of the foam-mattress-in-a box types have the fiberglass, though most of them disclose the presence of the fiberglass rather than hiding it like a dirty secret. Make sure you do a search for mattresses WITHOUT fiberglass as a flame retardant.
I had to go back and find this post because we just discovered our (Zinus) mattress is leaking fiberglass, and we NEVER removed or even touched the zipper on the cover.
My partner had changed the sheets, and then later while outside we saw that he was covered in shiny fiberglass (like the video above). I remembered this post and immediately knew we had to check the mattress. Sure enough there were glittery fibers EVERYWHERE in the bedroom, all over the floor, sheets & laundry, etc.
We are still trying to figure out just how bad the damage is & how much we need to throw away vs. what can maybe be salvaged.
Again, we NEVER removed the cover. And there is no evidence of the cover having been damaged anywhere.
It just was 3-4 years of regular use and then suddenly, one day while changing the sheets, there was glass everywhere. It’s probably been leaking into our laundry, and likely our bodies, for who knows how long.
Lots of people saying these mattresses are safe as long as you don’t remove the cover - it’s NOT true. Maybe it’s fine for a year or two, but at some point the fibers break down and start to come out THROUGH the cover.
These mattresses are outrageously dangerous & they should not be allowed to keep selling them. Yet they are one of the top selling brands on Amazon…
“We all occupy our own bubbles. Trust in others, even our neighbors, is at an historic low. Much of society has become like an airplane boarding line, with different rights and privileges for zones one to ninety-seven, depending on your wealth, frequent-flier miles, credit rating, and S.A.T. scores; and many of those in line think—though no one likes to admit it—that they deserve what they have more than the others behind them. Then the boarding agent catches some people from zone eighty-four jumping ahead of the people in zone fifty-seven, and all hell breaks loose.
Insisting that people are equally worthy of respect is an especially challenging idea today. In medicine, you see people who are troublesome in every way: the complainer, the person with the unfriendly tone, the unwitting bigot, the guy who, as they say, makes “poor life choices.” People can be untrustworthy, even scary. When they’re an actual threat—as the inmate was for my chief resident—you have to walk away. But you will also see lots of people whom you might have written off prove generous, caring, resourceful, brilliant. You don’t have to like or trust everyone to believe their lives are worth preserving.
We’ve divided the world into us versus them—an ever-shrinking population of good people against bad ones. But it’s not a dichotomy. People can be doers of good in many circumstances. And they can be doers of bad in others. It’s true of all of us. We are not sufficiently described by the best thing we have ever done, nor are we sufficiently described by the worst thing we have ever done. We are all of it.
Regarding people as having lives of equal worth means recognizing each as having a common core of humanity. Without being open to their humanity, it is impossible to provide good care to people—to insure, for instance, that you’ve given them enough anesthetic before doing a procedure. To see their humanity, you must put yourself in their shoes. That requires a willingness to ask people what it’s like in those shoes. It requires curiosity about others and the world beyond your boarding zone.
We are in a dangerous moment because every kind of curiosity is under attack—scientific curiosity, journalistic curiosity, artistic curiosity, cultural curiosity. This is what happens when the abiding emotions have become anger and fear. Underneath that anger and fear are often legitimate feelings of being ignored and unheard—a sense, for many, that others don’t care what it’s like in their shoes. So why offer curiosity to anyone else?
Once we lose the desire to understand—to be surprised, to listen and bear witness—we lose our humanity. Among the most important capacities that you take with you today is your curiosity. You must guard it, for curiosity is the beginning of empathy. When others say that someone is evil or crazy, or even a hero or an angel, they are usually trying to shut off curiosity. Don’t let them. We are all capable of heroic and of evil things. No one and nothing that you encounter in your life and career will be simply heroic or evil. Virtue is a capacity. It can always be lost or gained. That potential is why all of our lives are of equal worth.”
It is so easy these days to hide an eating disorder behind the guise of “healthy living” or a passion for health food and exercise. Actually, most people with eating disorders hide the eating disorders from themselves under the guise of healthy living. Yep! Most people with eating disorders don’t even know they have eating disorders until they are way into the disorder.
Forming a healthy relationship with food is so important and so difficult. If you are interested in reading more about our relationship with eating, The Fat Nutritionist is a great resource.
“I spent a lot of time babysitting [my siblings] as a teenager and I think it’s been a challenge for me to separate out feeling like I’m a parent to them.”
This has often caused rifts between the siblings into adulthood, Rosenfeld says. “I’ve always been somebody who thinks it’s my job to offer help, care, and advice even when it’s not asked for.”
How does someone learn that becoming self-reliant is safer than trusting others? Nakazawa believes that in destructive parentification, “you don’t have a reliable adult to turn to.” And if a child’s early experiences at home consisted of making sure everyone else’s needs were met, then the “child doesn’t feel seen.
This sense of responsibility and compulsive caretaking can follow them into future relationships as well. “You tend to project it onto other people in your life,” Rosenfeld says. This isn’t surprising, claims Jenny Macfie, an associate director of clinical training at the University of Tennessee and another prominent parentification researcher, as “adults who report role confusion in their childhoods may have difficulty with their identity development,” and this in turn, can affect a person’s romantic relationships.
We’re only beginning to understand the interplay between sibling dynamics, parental neglect, and health outcomes later in life. We need to see more research on prevention and treatment options.
This is a really smart idea - raising awareness of the proper use of 911 is essential in order to reduce wait times for those in need by avoiding unnecessary interventions that do not require first responders.
The premise of the pop-up restaurant, which was in a trial period from June 2 – June 4, 2017, was that the staff who have dementia may get your order wrong. But if you go in knowing this upfront, it changes your perception about those who suffer from brain disease. The experience makes you realize that with a little bit of understanding on our part dementia patients can be functioning members of society.
Food blogger Mizuho Kudo visited The Restaurant of Order Mistakes and had a blast. She originally ordered a hamburger but ended up having gyoza dumplings instead, but everything turned out to be unexpectedly delicious. Kudo also claimed that the waiters were full of smiles and seemed to be having tons of fun.
It’s great to see people with dementia living full lives and contributing to their communities!
The idea is this: If some people are going to use heroin no matter what, it’s better to give them a safe source of the stuff and a safe place to inject it, rather than letting them pick it up on the street — laced with who knows what — and possibly overdose without medical supervision. Patients can not only avoid death by overdose but otherwise go about their lives without stealing or committing other crimes to obtain heroin.
And it isn’t some wild-eyed theory; the scientific research almost unanimously backs it up, and Crosstown’s own experience shows it can make a difference in drug users’ lives.
Notions of willpower are easily stigmatizing: It becomes OK to dismantle social safety nets if poverty is a problem of financial discipline, or if health is one of personal discipline. An extreme example is the punitive approach of our endless drug war, which dismisses substance use problems as primarily the result of individual choices.
Such a fantastic read on a topic that permeates our health and social systems.
We’re starting our “metabolism” module at med school this week, and I’m dreading it with every fibre of my being. You see, I am going to be a doctor, and I am fat.
I’m not the type of fat you feel after you’ve had a big lunch, and your usually flat belly is protesting against the waistband of your jeans. I’m the real kind. My BMI hovers a couple of points below “morbidly obese”.
I worry a lot about what people will think of me as a fat doctor. For the smartarses among you, of course I’ve tried to be non-fat, it goes without saying. The thing is though, bodies don’t really like weighing less all of a sudden and are pretty good at reversing things in the long run. Mostly my body settles back to the same size 18 shape eventually.
I am always aware of my fatness, but perhaps more so here at medical school. We are training to work with bodies, and mine is a type of body we warn our patients not to have. It is the first thing described in every list of ‘modifiable risk factors’. A colleague suggests “just don’t let yourself get too fat” as we talk about preventing a certain type of cancer. A final exam question asks us to list four poor health outcomes associated with obesity. I sit through lectures with slides that have sniggering titles like “how BIG is the problem?”
For the first time during his hospital stay, his pain became real to me, and I realized I had wronged my patient by not taking his complaints more seriously. We gave him an opioid for his pain, and, slowly, the pain in his finger improved.
We’re taught in medical school not to undertreat pain, yet we do it too often in our zeal to not promote addiction. But many people who misuse opioids started out seeking pain treatment. We’re not doing enough, but what more can we do?
Don’t get me wrong. We absolutely need to continue to ask questions. We need to be more responsible when we prescribe these powerful drugs. And, yes, we need to remain vigilant for any signs of drug-seeking behavior.
That said, we have to be a little more trusting of our patients when it comes to their pain. Getting better control of their pain may help them recover faster and stay healthier longer.
With the opioid overdose epidemic, there is a palpable resurgence of very conservative pain management. We need to recognize that some people need opioids for pain management. Ultimately, substance use disorders and overdose are largely driven by disconnection, trauma, and stigma surrounding drug use, not the drugs themselves. Let’s evaulate and change the environments within which people are using drugs (i.e. address the social determinants of health, including employment, education, housing, and income). Limiting the conversation to restricting people’s access to medications obstructs a larger conversation on how our environments shape health behaviours.
“Hospice is not about dying. It is about living the remainder of your life how you want to. Not how I want you to, not how your husband, wife, daughters, or sons want you to, and not how the doctor wants you to, but how you want to.”
Sometimes, the way we frame something makes all the difference.




















 — Veloso Salgad")























